Download
1 / 21
210 likes | 380 Views
Project UPLIFT. Nancy J. Thompson, Ph.D., M.P.H. Rollins School of Public Health Emory University. Project UPLIFT. U sing P ractice and L earning to I ncrease F avorable T houghts Delivery of mindfulness-based cognitive therapy by telephone and Internet To people with epilepsy

E N D
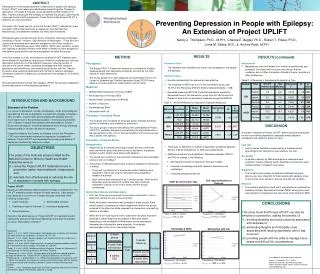
Project UPLIFT Nancy J. Thompson, Ph.D., M.P.H. Rollins School of Public Health Emory University
Project UPLIFT • Using Practice and Learning to Increase Favorable Thoughts • Delivery of mindfulness-based cognitive therapy by telephone and Internet • To people with epilepsy • Most of the work presented here was funded by the Centers for Disease Control and Prevention
About Mindfulness-based Cognitive Therapy (MBCT) • Cognitive Therapy addresses the unrealistic thinkingassociated with depression. • Uses verbal techniques to explore the reasoning behind specific attitudes and assumptions. • Client is taught to recognize, monitor, and record negative thoughts on a daily record. • CBT focuses on changing thought content while mindfulness changes relationship to the thoughts—see them as passing events that do not necessarily represent a state of reality. • Mindfulness is important in preventing relapse.
Cognitive Therapy vs. Medications in the Treatment of Moderate to Severe Depression Across the 3 treatments ([chi]22 = 10.22, P = .006). ADM vs. pill placebo ([chi]21 = 10.17, P = .001), CT vs. pill placebo ([chi]21 = 4.44, P = .04) ADM vs. CT ([chi]21 = 0.71, P = .40). Between sites: Wald [chi]22 = 1.59, P = .45
Follow-up after Mindfulness vs. Treatment as Usual for the Treatment of Depression 4+ Sessions Intent to Treat
Project UPLIFT • Delivery of MBCT by Web and Telephone Groups • People with epilepsy randomly assigned to groups of 7 • Initially computers and Internet access provided if needed • Group delivery important for support surrounding epilepsy • Co-Facilitators • Graduate Public Health Student • Person with epilepsy • Supervised by a licensed psychologist
Potential Benefits • Cost-effective • Can reach the mobility/transportation limited • Equal reach to urban and rural • Allows peer support, even with rare conditions • Potential for anonymity and avoidance of stigma • Can prevent relapse • Does not require more medication • Mindfulness may improve attention/cognition
Project UPLIFT • 8 Sessions (1 hour by phone) • Noting Challenging/Changing Impermanent
Telephone Version Session Four: Attention and Mindfulness
Web Version Session One: Monitoring Thoughts
Formative Evaluation Focus Groups • Importance of Group • “Medical professionals can tell you the what, the why, the diagnosis, but in a group of people with epilepsy, there’s camaraderie and you can see what other people go through.” • “Being in a group with other people with epilepsy is like sharing with your close friends. You realize that everyone has their insecurities and you feel more safe.” • Response to Activities • “If I could learn to modify my thoughts, that would be practical.” • “The good thing about doing mindfulness of sounds and thoughts is that you can do it anywhere.”
Design—Outcome Evaluation Stratum 1:Pretest 6-8 wk phone Interimas usual Follow-up Stratum 2:Pretest 6-8 wk Web Interimas usual Follow-up Stratum 3: Pretestas usual Interim 6-8 wk phone Follow-up Stratum 4: Pretestas usual Interim 6-8 wk Web Follow-up Baseline Week 8 Week 16
Depression: BDI • UPLIFT vs.Waitlist (treatment as usual) • Foverall = 42.22, p=.0001 • Finteraction= 11.99, p=.001*
Depression: BDI By Intervention Type • Phone vs. Web vs. Waitlist (treatment as usual) • Foverall = 41.65, p=.0001 • Finteraction= 5.93, p=.006*
No difference with • Major Depressive Disorder or not (F1,35= 1.21, p = 0.279) • Maintenance
Knowledge/Skills & Self-Efficacy
Quality of Life 1.05<p<.10
Summary • Effective in: • Reducing depressive symptoms and teaching knowledge and skills associated with reducing depression • Intervention group showed significant improvement compared to the waitlist • Equally effective for those with and without MDD • Reduction in depressive symptoms maintained • Approaching significance for Satisfaction with Life and Depression Coping Self-Efficacy • Delivery • Both phone and web were significantly more effective in reducing depression than waitlist condition
Participants’ Comments • “I told my therapist I think I like this way a lot better…I’ve always went and talked to somebody versus learning to work through things just using my own mindset.” • “The project had great value. I'm thankful that I was able to participate. I got a lot out of the exercises and coping skills.” • “The program was very helpful and that surprised me. I printed everything out and recorded the meditations onto my MP3 player.” • “The program helped me more than the antidepressants I've been on for years.” • “Thank you for helping me because I have been depressed and now I can cope.”
Potential Benefits • Cost-effective • Reaches the mobility limited • Equal reach to urban and rural • Can form groups even with rare conditions • Potential for anonymity and avoidance of stigma • Prevent relapse
Project UPLIFT • Next Phase • ~$1 million Challenge Grant • UPLIFT for Prevention • Participants in MEW network states • Georgia • Michigan • Texas • Washington