Download
1 / 1
10 likes | 128 Views
ABSTRACT

E N D
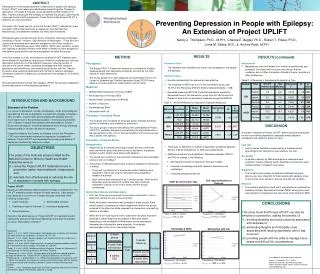
ABSTRACT Developed for home-based treatment of depression in people with epilepsy, Project UPLIFT was based upon Mindfulness-based Cognitive Therapy for depression. It includes 8 modules, group-delivered by either telephone or Web. Trainees and people with epilepsy co-facilitate the groups, supervised by a licensed mental health professional. These factors make Project UPLIFT a relatively low-cost intervention. The goals of this study were to: revise the Project UPLIFT materials for use in prevention (rather than treatment) of depression and estimate their effectiveness; and determine whether any effect was maintained. Participants were recruited through: Emory University, University of Michigan, University of Texas—Houston, and University of Washington. Those who met criteria and consented were randomly assigned to one of two conditions: UPLIFT or a Treatment-as-usual (TAU) waitlist. Within each condition, people who required a particular delivery mode (Web or telephone) were assigned to that delivery group and the rest were assigned to equalize the groups. In the final sample (n=108), the prevention-modified UPLIFT materials were found effective in significantly: reducing the incidence of depression; reducing depressive symptoms on three different measures; reducing number of seizures in the past 4 weeks; increasing knowledge and skills related to depression and mindfulness; and increasing satisfaction with life. Results showed a dose-response relationship with number of sessions attended. Decreased symptoms of depression persisted over the average of 10.5 weeks of follow-up. Although developed for people with epilepsy, UPLIFT can easily be adapted to prevent depression in other disparity populations. Preventing Depression in People with Epilepsy:An Extension of Project UPLIFT  Nancy J. Thompson, Ph.D., M.P.H., Charles E. Begley, Ph.D., Robert T. Fraser, Ph.D., Linda M. Selwa, M.D., & Archna Patel, M.P.H. RESULTS • METHOD • Participants • The Project UPLIFT Preventive Intervention is intended for English-speaking people with depressive symptoms, but who do not meet criteria for major depression. • The first 42 people from each state who scored between 9-26 on the Center for Epidemiologic Studies Depression Scale (CES-D)were asked to provide consent for randomization into the study. • Measures • Modified Beck Depression Inventory (mBDI) • Beck Depression Inventory (BDI) • Patient Health Questionnaire-9 (PHQ-9) • Number of Seizures • Knowledge and Skills • Satisfaction with Life • Procedure: Formative Phase • The modules were reviewed for language and/or activities that were specific to treatment, and modified for prevention. • Two focus groups of people with epilepsy who participated in Project UPLIFT for treatment assisted in re-evaluating the appropriateness of the revised intervention. One of the two facilitators of the focus groups was a person with epilepsy. • Procedure: Outcome Phase • Randomization • Supervised by a licensed clinical psychologist at Emory University, each intervention group was lead by two co-facilitators: a graduate student in public health and a person with epilepsy. • The impact and outcome of the prevention intervention were assessed using a cross-over design.6 • A maximum of 168 participants were randomly assigned to intervention or waitlist. • Those with a preference for a particular mode of delivery were assigned to that mode, and the remainder were assigned to equalize the groups. • Each stratum was comprised of six 7-person groups. After the first 28 people were recruited from a state, they were randomly assigned to a group in one of four strata, and the groups commenced. • Intervention Delivery and Assessment • First, two of the groups received the prevention intervention: one by telephone conference call, and one by Web. • When the 8-week intervention was complete in these groups, there were 3 weeks to complete the interim assessment before the groups assigned to the other two strata received the intervention; one each by telephone and Web. • When the final 14 participants from a state were recruited, they were assigned to either telephone and waitlist or Web and waitlist, depending on the availability of Web access for the participants; thereafter they followed the same schedule. A schematic representation of the cross-over design follows: • RESULTS (continued) • Maintenance • Maintenance over the 8 weeks from interim to posttest was also assessed. Consistent with the cross-over design, the two conditions did not differ at baseline, differed at interim, and did not differ at follow-up. • Table 2. Differences in Depressive Symptoms by Time • DISCUSSION • A number of features of Project UPLIFT make it particularly attractive for use in preventing depression, especially among disparity populations with regard to access to care. • Low cost • Led by trained facilitators supervised by a licensed clinical psychologist, this intervention was relatively low cost. • Accessible • In addition, delivery by Web and telephone reduced access problems, thereby reducing health disparities for those who were mobility-limited or located in rural areas. • Supportive • The formative and process evaluations indicated that group delivery was very important for these people with epilepsy, many of whom had never spoken to anyone else with the condition. • Effective • The outcome evaluation found that it was effective in reducing the incidence of Major Depressive Disorder (MDD) among those who had symptoms of depression but did not yet meet criteria for MDD. • Formative Phase • The materials were modified and found to be acceptable to the people with epilepsy. • Outcome Phase • Results indicated that the intervention was effective. • The incidence of MDD was 0.0% in the intervention group, and 10.7% in the TAU group (Fisher’s Exact 2-tailed probability = .028). • Repeated measures ANCOVA found that depressive symptoms decreased more in the intervention group than the TAU group from Pretest to Interim for all depression measures except the NDDI-E. • Table 1. ANCOVA Results for Depressive Symptom Measures • There was no difference in change in depressive symptoms between delivery method of telephone vs. Web (see graph below). • Additional analyses found significant differences between UPLIFT and TAU for change in the following: • Self-reported number of seizures in the past 4 weeks • Increase in knowledge and skills related to depression and mindfulness • Increased satisfaction with life INTRODUCTION AND BACKGROUND Statement of the Problem In a review of depression, suicide, and epilepsy, Jones and colleagues1 reported that the rate of depression in people with epilepsy is between 32% and 48%. Suicide rates among people with epilepsy also are much higher than in the general population. One study reported that 14% of deaths in people with epilepsy were attributable to suicide. 2 Boylan and colleagues 3 found that depression more strongly predicted reduced quality of life than did seizure frequency. Originally funded by the Centers for Disease Control and Prevention (CDC) as a home-based treatment for depression in people with epilepsy, Project UPLIFT was developed to provide group delivery of depression treatment by telephone or Web. Project UPLIFT Based upon Mindfulness-based Cognitive Therapy for Depression,4 the UPLIFT materials include modules for eight sessions. Each session was designed to be one hour in length and was comprised of the following components: Results of the effectiveness of Project UPLIFT for treatment found it significantly reduced symptoms of depression more than a treatment-as-usual (TAU) waitlist condition.5 • OBJECTIVES • The goals of this multi-site project funded by the National Center for Minority Health and Health Disparities were to: • revise the Project UPLIFT materials for use in prevention (rather than treatment) of depression; and • estimate their effectiveness in reducing the risk of depression in people with epilepsy. Self-reported Number of Seizures mBDI by Intervention Type Check-in period Teaching on topic of the week Group discussion Skill-building exercise Homework assignment • CONCLUSIONS • This study found that Project UPLIFT can also be effective for prevention, adding the benefits of: • avoiding disability and lost productivity associated with depression;7 • eliminating tangible and intangible costs associated with treating depression after it has occurred; • providing people with the skills to manage future stress and difficult life circumstances. Phone vs. Web vs. Waitlist Finteraction= 3.46, p=.035 Treatment vs. TAU Waitlist Finteraction= 5.178, p = 0.025 Knowledge & Skills Satisfaction with Life References:1Jones, J. E. et al. (2005). Screening for major depression in epilepsy with common self-report depression inventories. Epilepsia, 46, 731-735. 2Fukuchi, T. et al. (2002). Death in epilepsy with special attention to suicide cases. Epilepsy Research, 51, 233-236. 3Boylan, L. S. et al. (2004). Depression but not seizure frequency predicts quality of life in treatment resistant epilepsy. Neurology, 62, 258-261. 4Segal, Z. V. et al. (2002). Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse. New York: Guilford. 5Thompson, N. J. et al. (2010). Distance delivery of mindfulness-based cognitive therapy for depression: Project UPLIFT. Epilepsy & Behavior, 19, 247-254. 6Thompson, N. J., & McClintock, H. O. (1998). Demonstrating your program’s worth: a Primer on evaluation for programs to prevent unintentional injury. Atlanta: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. 7Gillham, J. et al. Preventing depression: A review of cognitive-behavioral and family interventions.Appl & PrevPsychol, 2006 (9): p. 63-88. For additional information please contact: Nancy J. Thompson, Ph.D., M.P.H. Behavioral Sciences and Health Education Rollins School of Public Health, Emory University nthomps@emory.edu Treatment vs. TAU Waitlist Finteraction= 4.184, p = 0.043 Treatment vs. TAU Waitlist Finteraction= 7.898, p = 0.006