Download
1 / 1
10 likes | 127 Views
Multi-Institutional Audit of octaplex ® & Comparison with National Recommendations S. Nahirniak, J. Callum, C. Doncaster, Y. Lin, M.C. Poon, L. Whitman On Behalf of the PCC Working Group of the National Advisory Committee on Blood & Blood Products of Canada*. Conclusion. Background. Results.

E N D
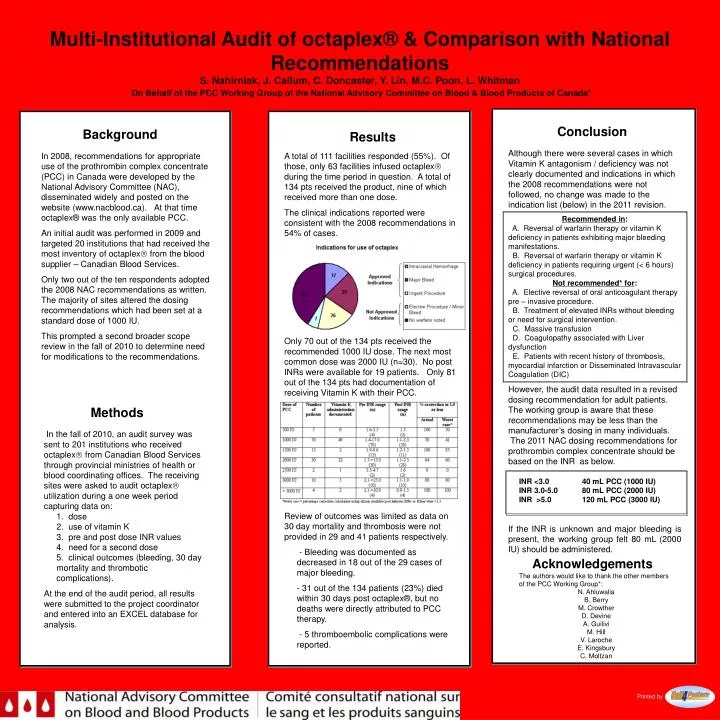
Multi-Institutional Audit of octaplex® & Comparison with National RecommendationsS. Nahirniak, J. Callum, C. Doncaster, Y. Lin, M.C. Poon, L. WhitmanOn Behalf of the PCC Working Group of the National Advisory Committee on Blood & Blood Products of Canada* Conclusion Background Results Although there were several cases in which Vitamin K antagonism / deficiency was not clearly documented and indications in which the 2008 recommendations were not followed, no change was made to the indication list (below) in the 2011 revision. Recommended in: A. Reversal of warfarin therapy or vitamin K deficiency in patients exhibiting major bleeding manifestations. B. Reversal of warfarin therapy or vitamin K deficiency in patients requiring urgent (< 6 hours) surgical procedures. Not recommended* for: A. Elective reversal of oral anticoagulant therapy pre – invasive procedure. B. Treatment of elevated INRs without bleeding or need for surgical intervention. C. Massive transfusion D. Coagulopathy associated with Liver dysfunction E. Patients with recent history of thrombosis, myocardial infarction or Disseminated Intravascular Coagulation (DIC) However, the audit data resulted in a revised dosing recommendation for adult patients. The working group is aware that these recommendations may be less than the manufacturer’s dosing in many individuals. The 2011 NAC dosing recommendations for prothrombin complex concentrate should be based on the INR as below. INR <3.0 40 mL PCC (1000 IU) INR 3.0-5.0 80 mL PCC (2000 IU) INR >5.0 120 mL PCC (3000 IU) If the INR is unknown and major bleeding is present, the working group felt 80 mL (2000 IU) should be administered. In 2008, recommendations for appropriate use of the prothrombin complex concentrate (PCC) in Canada were developed by the National Advisory Committee (NAC), disseminated widely and posted on the website (www.nacblood.ca). At that time octaplex® was the only available PCC. An initial audit was performed in 2009 and targeted 20 institutions that had received the most inventory of octaplex from the blood supplier – Canadian Blood Services. Only two out of the ten respondents adopted the 2008 NAC recommendations as written. The majority of sites altered the dosing recommendations which had been set at a standard dose of 1000 IU. This prompted a second broader scope review in the fall of 2010 to determine need for modifications to the recommendations. • A total of 111 facilities responded (55%). Of those, only 63 facilities infused octaplex during the time period in question. A total of 134 pts received the product, nine of which received more than one dose. • The clinical indications reported were consistent with the 2008 recommendations in 54% of cases. • Only 70 out of the 134 pts received the recommended 1000 IU dose. The next most common dose was 2000 IU (n=30). No post INRs were available for 19 patients. Only 81 out of the 134 pts had documentation of receiving Vitamin K with their PCC. • Review of outcomes was limited as data on 30 day mortality and thrombosis were not provided in 29 and 41 patients respectively. • - Bleeding was documented as decreased in 18 out of the 29 cases of major bleeding. • - 31 out of the 134 patients (23%) died within 30 days post octaplex®, but no deaths were directly attributed to PCC therapy. • - 5 thromboembolic complications were reported. Methods • In the fall of 2010, an audit survey was sent to 201 institutions who received octaplex from Canadian Blood Services through provincial ministries of health or blood coordinating offices. The receiving sites were asked to audit octaplex utilization during a one week period capturing data on: • 1. dose • 2. use of vitamin K • 3. pre and post dose INR values • 4. need for a second dose • 5. clinical outcomes (bleeding, 30 day mortality and thrombotic complications). • At the end of the audit period, all results were submitted to the project coordinator and entered into an EXCEL database for analysis. Acknowledgements The authors would like to thank the other members of the PCC Working Group*: N. Ahluwalia B. Berry M. Crowther D. Devine A. Guilivi M. Hill V. Laroche E. Kingsbury C. Moltzan Printed by






















