Download
1 / 29
370 likes | 1.06k Views
Abdomen Assessment. D. Tanner, RN, MSN NUR 211 Fall Semester. Anatomy of the Abdomen. 4 Quadrants RUQ, RLQ, LUQ, LLQ Midline 9 Regions- epigastric, umbilical, suprapubic

E N D
Abdomen Assessment D. Tanner, RN, MSN NUR 211 Fall Semester
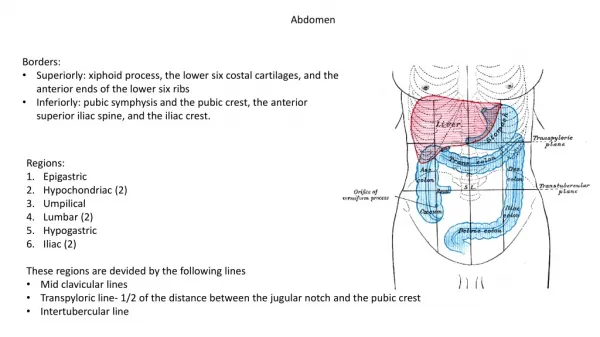
Anatomy of the Abdomen • 4 Quadrants RUQ, RLQ, LUQ, LLQ • Midline • 9 Regions- epigastric, umbilical, suprapubic The word "abdomen" has a curious story behind it. It comes from the Latin "abdodere", to hide. The idea was that whatever was eaten was hidden in the abdomen.
Location! Location! Location! • RUQ liver gallbladder duodenum (small intestine) pancreas head right kidney and adrenal
Location! Location! Location! • RLQ cecum appendix right ovary and tube
Location! Location! Location! LLQ sigmoid colon left ovary and tube LUQ stomach spleen pancreas left kidney and adrenal
GI Variations Due to Age • Aging- should not affect GI function unless associated with a disease process • Decreased: salivation, sense of taste, gastric acid secretion, esophageal emptying, liver size, bacterial flora • Increased: constipation!
GI Variations with pregnancy • Decrease in gastric motility • High incidence of N, V (r/t pregnancy hormones) and “heartburn” or acid reflux • Bowel sounds diminished r/t enlarged uterus displacing intestines • Linea nigra- increased pigmentation of abd midline • Striae Gravidarum
Nursing History - Abdomen • Subjective Data: Ask about: Appetite Wt gain or loss Dysphagia Intolerance to certain foods Any Abdominal Pain of Nausea and Vomiting Bowel movements Any past abdominal problems
Nursing History • Infants and Children – • Ask: bottle or breast fed, any table foods, how often & how well & how much the baby eat, any problems with constipation, c/o of any abdominal pain • Teenagers- • Ask: nutritional assessment, activity & exercise patterns, recent wt. loss or gain
Nursing History • Older Adults • Ask: how do you get your groceries? prepare your meals? do you have any trouble swallowing? how often do your bowels move? how often do you take anything for constipation? Rx / OTC/ herbs what meds do you take?
Nursing Assessment • Objective Data: General Observation Inspect Auscultate Percuss Palpate (always last)
Focused Health History • Nutrition • Allergies • Medications • Cigarette/tobacco • ETOH intake • Recreational drug use • Stool characteristics • Urine characteristics • Exposure to infectious dz. • Recent stressful life events • Possibility of Pregnancy
Techniques for Exam • Provide privacy • Good lighting/appropriate temp in rm • Expose the abdomen • Empty bladder • Position pt supine, arms by side & head on pillow with knees slightly bent or on a pillow • Warm stethoscope & hands • Painful areas last • Distraction techniques
Inspection • Overall observation • Abd contour- flat, scaphoid, round, protuberant • Abd symmetry and skin color - note any masses, striae, scars, veins, pigmentation • Pulsations
Auscultation • Always done before percussion & palpation • Use diaphragm of stethoscope • Listen lightly • Start with RLQ
Auscultation • What makes a bowel sound? • Note character & frequency of bowel sounds (5-30 times/minute) • Sounds like….. • Listen for 5 minutes before documenting absent bowel sounds • Listen for bruits- aortic, renal, iliac, femoral • Hyper- gastroenteritis, obstruction, hungry • Hypo- pregnancy, peritonitis
Percussion • Gently tapping on the skin to create a vibration • Detect fluid, gaseous distention and masses • Tympany- gas (dominant sound because of air in sm intestine) • Dullness- solid masses, distended bladder • Percuss liver, spleen ,kidneys
Palpation of Abdomen • Light palpation- depress about 1 cm. Assess skin pulsations. Always done first- clockwise • Deep palpation- depress skin about 5-8 cm. • Always assess tender areas last. • Watch pt’s expression during palpation
Inspection Abnormal Findings • Visible or distended veins- ascites • Visible peristalsis- obstruction • Spider nevi (cutaneous angiomas)- cirrhosis • Asymmetry/ Distention- mass or intestinal obsruction • Color changes- jaundice, bluish/cyanotic
Abnormal Auscultation • Absence/Hyperactive bowel sounds- “borborygmi” • Bruits- “swoosh” • Peritoneal Friction Rub- rough, grating heard over liver & spleen- inflammation of peritoneal surface from tumor, infection, etc.
Percussion Abnormal Findings • Enlarged organs, palpable masses, distention, ascites • Marked tenderness
Palpation Abnormal Findings • Tenderness- rebound- done away from painful area- done at end of exam • Masses- document location, size, shape, mobile, pulsating, smooth, nodular, firm • Firmness or muscle guarding/rigidity- intraabdominal bleeding- DO NOT CONTINUE TO PALPATE!!!!!!
Special Procedures • Fluid Wave- need 3 hands- feel for impulse of the wave of fluid across the abdomen= ascites • Rebound Tenderness- Blumberg’s Sign • Iliopsoas Muscle Test- thigh muscle lift R leg and push down on R thigh= appendicitis • Obturator Test- lift R leg and rotate at 90 degrees= muscle is irritated by appendicitis • Murphy’s Sign- “inspiratory arrest” palpate the liver should be painless= cholecystitis
Special Procedures • McBurney’s Point- RLQ midclavicular= appendicitis • Referred pain- location of pain is not necessarily where the involved organ is! May be felt where the organ was located in fetal development ex: spleen= L shoulder pain/ kidney= groin pain • Hooking technique- palpate the liver- feeling for the liver edge
Special Procedures • Cullen’s Sign- bluish discoloration around the umbilicus EMERGENCY!!! • Kehr’s Sign- abd pain radiating to R shoulder= spleen or pancreatitis
Sample Documentation • Normal Exam- Abdomen soft, rounded and symmetric without distention; no lesions or scars, or visible peristalsis. Aorta midline without bruit or visible pulsation; umbilicus inverted and midline without herniation; bowel sounds present in all 4 quadrants. Liver, kidney and spleen non-palpable; no tenderness on palpation. Reports good appetite; no constipation, nausea or diarrhea. Voiding well and denies laxative use.