Download
1 / 29
390 likes | 1.46k Views
Adenotonsillar hypertrophy (ATH) 0bstructive Sleep apnea (OSA). Yosseph Rosen M.D. Head of Pediatric Health Center Kfar Saba. Q&A. miok.co.il שאלה מתאריך 06.10.2003 בני בן 4, נוחר בשנתו ובצילום נראה פוליפ מוגדל. היינו אצל 2 רופאי א.א.ג

E N D
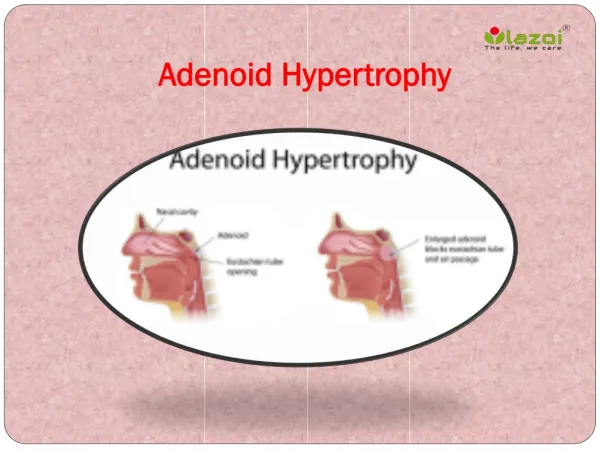
Adenotonsillar hypertrophy (ATH)0bstructive Sleep apnea (OSA) Yosseph Rosen M.D.Head of Pediatric Health Center Kfar Saba
Q&A miok.co.il שאלה מתאריך06.10.2003 • בני בן 4, נוחר בשנתו ובצילום נראה פוליפ מוגדל. • היינו אצל 2 רופאי א.א.ג • הראשון לא המליץ לנתח מאחר והילד אינו עושה הפסקות נשימה (עשה בעבר) • והרופא השני אמר מיד לנתח ! . • מה לעשות? • האם לא לנתח יזיק לבריאותו של הילד? • אולי יש כרית מיוחדת שתעזור והאם יש חשיבות בכלל לסוג וגודל כרית לילדים?
Adenoids Unclear Guidelines Delayed Diagnosis And Treatment
Adenoid Hypertrophy Mild • Difficulty of breathing • Rec. URTI • Rec. Otitis Media • Ear effusion not persistent • X- rays: mild adenoid hypertrophy
Sleep history: • Snoring • Restlessness • Frequent arousals • Peculiar sleep position • Refuse pacifier during sleep • Sleeping with open mouth • Sleep apnea • Sleepy during the day
Basic considerations OSAS • Chronic sleep-related airway obstruction • Muscular hypotonia • Repetitive brain hypoxemia • Sleep pattern disturbances • Neurocognitive disturbances • Growth and developmental failure
Obstructive Apnea in Children - definition • By time : • 5-20 sec. • Any pause of breath that produces desaturation • SaO2 > 89% • A drop of 4% in SaO2
OSA & Hypoventilation Epidemiology: • 1% of pediatric population • Children of ALL AGES • Peak incidence 2-6 years • Positive family history • Risk factors: Chronic rhinitis Asthma Obesity
OSA in children • Infants: • Cong. Syndromes • Malformations • Children: • Adenoid hypertrophy
OSA in children Predisposing factors Anatomical Functional
OSAS & Hypoventilation Etiology – Predisposing factors: Anatomical factors: • Choanal atresia / stenosis • Deviated nasal septum • Severe allergic rhinitis • Adenotonsillar hypertrophy • Macroglossia • Cleft palate repair • Congenital craniofacial anomalies
OSA & Hypoventilation Etiology – Predisposing factors: Anatomical factors:INFANTS • Congenital Craniofacial anomalies • Micrognathia (isolated or syndromes) • Macroglossia - Down’s Syn., MPS • Mid-face hypoplasia: Crouzon, Apert • Muscular dystrophy • Werdnig - Hoffman
OSA & Hypoventilation Etiology – Predisposing factors: Functional factors: • REM sleep + Pharyngeal hypotonia • CNS injury (CP, Birth asphyxia) • Drugs: phenothiazines, chloral hydrate Narcotics • Dysphagia • Obesity • Prematurity • Excess oral secretions
Adenotonsillar hypertrophy ininfants • Symptoms:c • Snoring • Restlessness while sleeping • Frequent arousals / crying • Intermittent sleep apnea • Tired in the morning • Dysphagia • Failure to thrive
ATH Infants • Complications • Failure to thrive • Growth retardation • Developmental delay • Post surgery • Complete recovery • Recurrence 24%
Adenoid Hypertrophy in Children • Symptoms: • Chronic rhinitis • Mouth breathing (mostly at night) • Mouth open during day (severe obstruction) • Halitosis • Dry mouth / Cracked lips • Frequent OM • Snoring • Restlessness while sleeping • Intermittent sleep apnea
Adenotonsilar Hypertrophy • Severe symptoms: (Obstruction) • Mouth breathing (day time) • Rec. OM / Ch. Rhinitis / Rec. Sinusitis • ADHD like syndrome • Failure to thrive • Hyponasal speech • Adenoid facies • Cor pulmonale ? IMMUNITY DAYCARESMOKING ALLERGY
Adenoid Hypertrophy Differential diagnosis • Foreign body in the nose • Nasopharyngeal angiofibroma
Diagnosis of ATH in children • Clinical presentation + • Lat. Neck X-rays • Fiberoptic nasopharyngoscopy • Polysomnography • CT • MRI
Therapy of ATH in children • SURGERY • Corticosteroids • Antihistamins • Decongestants • Antibiotics • CPAP
Nasal spray corticosteroids4 different controlled trials • Drug, dose, duration of therapy, • Presenting complaint and disease severity, • Method of quantitating ATH , • presence of coexistent tonsillar hypertrophy, • presence of other medical conditions, • Effect on the nasal mucosa, • Relapse after discontinuing treatment, • Short follow up,
ATH • Complications • Failure to thrive • Growth retardation • Hyponasal speech • Adenoid facies • Pulmonary hypertension • Cor pulmonale
Indications For tonsillectomy • Recurrent acute tonsillitis (7x/year) • Hypertrophy & sleep disturbance / apnea • Dental malocclusion • Orofacial growth malformations • Severe dysphagia • Cor pulmonale, • Rec. peritonsil. abscess • Chronic tonsillitis • Unilat. TH presumed neoplasm
Indications For Adenoidectomy • Hypertrophy causing airway obstruction • Sleep disturbance / apnea • Chronic nasal infection/ blockade • Rec. OM after first tubing • Persistent SOM • Dental malocclusion • Orofacial malformations • Severe dysphagia • Cor pulmonale
Indications ForAdenotonsillectomy • Rec. infections as for tonsillitis alone • Adenotonsillar hypertrophy & sleep disorder • Failure to thrive • Speech disturbences • Craniofacial abnormalities • Cor pulmonale (rare)
Adenotonsillar Hypertrophy Functional Definition Any adenoid and tonsillar enlargement that causes Airway obstraction (with Desaturation)
Adenotonsillar Hypertrophy • SNORING: • Heavy breating • Habitual snorers (Primary snoring) • Snoring during illness • Snoring as a part of OSAS
Adenotonsillar Hypertrophy Sleep history: • Snoring • Restlessness • Frequent arousals / irritable • Peculiar sleep position • Sleep apnea • Sleeping with open mouth • Refuse pacifier during sleep • Sleepy during the day
Obstructive Sleep Apnea Syndrome (OSAS) • Sleep Apnea • Obstructive apnea • Central apnea • Apnea / Hypopnea index • Apnea > ?