Download
1 / 18
260 likes | 588 Views
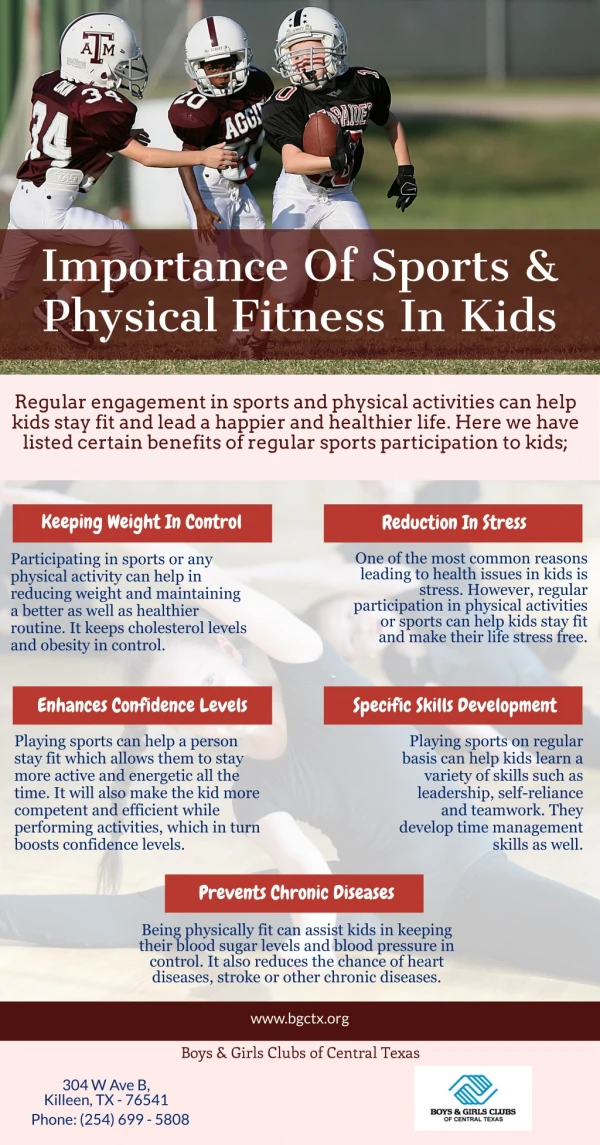
The Sports Physical. Valerie Robinson D.O. The Goals. The goal of the preparticipation sports physical is to maximize safety of participants. Identify life-threatening medical problems. Identify and treat other medical problems that may interfere with participation. (e.g. asthma, HTN)

E N D
The Sports Physical Valerie Robinson D.O.
The Goals • The goal of the preparticipation sports physical is to maximize safety of participants. • Identify life-threatening medical problems. • Identify and treat other medical problems that may interfere with participation. (e.g. asthma, HTN) • Identify previous injuries and try to prevent subsequent injuries • It does not substitute for a well child check.
The Exam • Most schools require annual physicals • Exam 4-6 weeks before sports season starts • May be done by the PCP • May be done in a station approach at locations set up by the school or local health department • Targeted medical hx • Targeted family hx • Target physical • Emphasis on musculoskeletal and cardiovascular • Labwork is not necessary
Given that 30-78% of adolescents have a sports physical in lieu of a well child check, it may be appropriate to take the time to perform a complete check-up as well. • If performed in a private office, the physician may ask about drug use, sexual activity, violence, and mental health (e.g. depression or bullying) as part of a comprehensive check-up
The History • Medical history • Seizure, excess fatigue, shob • Injury history • Where, when, lingering effects?, LOC • Pain, paresthesia, decreased ROM • Cardiovascular history • HTN, murmur, dyslipidemia, myocarditis, endocarditis, rheumatic fever, syncope, near-syncope, angina, palpitations • Family history • Especially cardiac or sudden death, Marfan’s, syncope, SIDS • Surgical history • Medications • Immunization history • Menstrual history • History of weight changes
The Physical • Vitals, BMI • Low BMI, bradycardia, hypotension, hypothermia are symptoms of an eating disorder • HEENT – need acuity test • If corrected acuity <20/40, need protective eyewear • Lungs - auscultate • Abdomen - splenomegaly • Genitals – testes, discuss cup • Skin – anything contagious? (herpes, varicella, scabies, tinea corpora, molluscumcontagiosum) • Lymphatic – lymphadenopathy, splenomegaly • Neuro – cranial nerves, focal defecits
The Physical The Cardiac Exam • Pulse and BP, right arm while sitting • Auscultation done supine and standing • Innocent murmur – systolic, decreases when standing • Hypertrophic cardiomyopathy – may have no murmur. Systolic, increases when standing and with Valsalva, decreases with squatting • Aortic stenosis – ejection murmur, split S2, murmur may radiate to carotids • Mitral prolapse – midsystolic click, poss late systolic murmur • Locate PMI • Asymptomatic bradycardia (40-50 bpm)may be present in fit athletes - does not preclude activity • EKG is not recommended for screening purposes
The PhysicalMusculoskeletal • If hx of injury, pay special attention to area involved • Look for asymmetry • Look for swelling, bruising, deformities • Watch for and ask about pain during exam • Test for weakness • Look for atrophy and watch for fasciculations
The PhysicalMusculoskeletal 2 • Shoulder • Full abduction, flexion, external rotation • Resisted flexion and abduction, apprehension test • Elbow • Flexion, extension, supination, pronation • Hands • Flexion and extension of fingers, grip strength • Neck • Flexion, extension, rotation, sidebending
The PhysicalMusculoskeletal 3 • Back • Look for scoliosis, spondylolysis • Flexion, extension, rotation • Hip • Flexion, extension, walk • “Duck walk” tests the hip and knee • Knee • Flexion, extension, walk, “duck walk” • Check for Osgood-Schlatter • Ankle • Hop several times on each foot
Tx Before Participating • HTN • DM 1 or 2 • Asthma • Exercise-Induced Bronchospasm • Dx by H&P. Spirometry or exercise challenge as indicated • Eating disorders • Treat psych. Cut exercise in half, esp. if 85% of IBW • Musculoskeletal injuries • Physical rehabilitation • Plan for return to activities. “Start low. Go slow.”
Relative Contraindications • Mitral prolapse – May participate UNLESS • Hx of syncope • Famhx of sudden death d/t prolapse • Arrhythmias • Moderate or greater mitral regurg • Hx of emboli • Uncontrolled HTN • Fever
Sudden Death • Sudden death in the young athlete occurs with a prevalence between 1:100,000 and 1:300,000. • 90% of deaths are in males, median age 17 • Causes: • Hypertrophic cardiomyopathy • Wolff-Parkinson-White – delta waves, SVT • Long QT syndrome • Aortic stenosis – more common in Marfan’s • Commotiocordis – precordial blow disrupts heart rhythm • Coronary artery anomalies • Right ventricular hypertrophy • Myocarditis • Aortic rupture
Refs • Albert C Hergenroeder, MD et al. “The preparticipation sports examination in children and adolescents.” UpToDate. Updated July 11, 2012. www.uptodate.com • Stephen G. Rice, MD, PhD, MPH et al. “Medical Conditions Affecting Sports Participation.” Pediatrics Vol. 121 No. 4 April 1, 2008 , pp. 841 -848. Retrieved from http://pediatrics.aappublications.org • Form: “Preparticipation Physical Evaluation Forms.” American Academy of Pediatrics. http://www.aap.org/en-us/professional-resources/practice-support/Pages/Preparticipation-Physical-Evaluation-Forms.aspx