Download
1 / 68
710 likes | 1.04k Views
The Respiratory System. The lower respiratory organs (larynx,trachea,bronchi,lungs) begin to develop during 4 th week , from laryngotracheal groove , which lies ventral to the caudal part of foregut (pharynx).

E N D
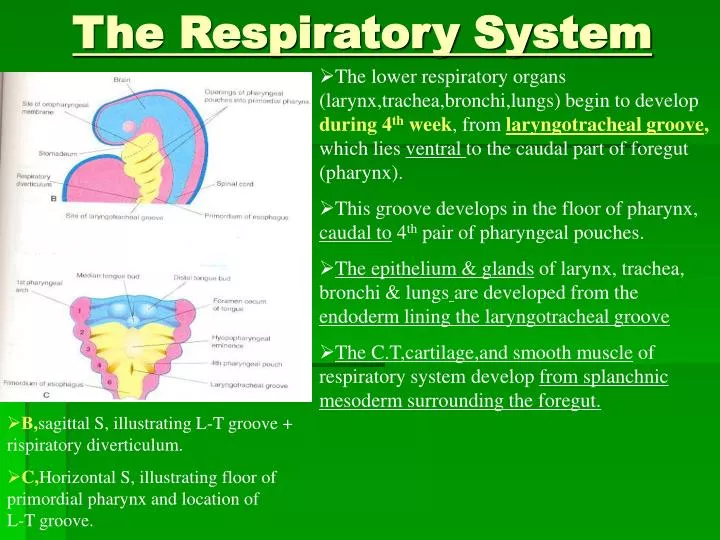
The Respiratory System • The lower respiratory organs (larynx,trachea,bronchi,lungs) begin to develop during 4th week, from laryngotracheal groove, which lies ventral to the caudal part of foregut (pharynx). • This groove develops in the floor of pharynx, caudal to 4th pair of pharyngeal pouches. • The epithelium & glands of larynx, trachea, bronchi & lungsare developed from the endoderm lining the laryngotracheal groove • The C.T,cartilage,and smooth muscle of respiratory system develop from splanchnic mesoderm surrounding the foregut. • B,sagittal S, illustrating L-T groove + rispiratory diverticulum. • C,Horizontal S, illustrating floor of primordial pharynx and location of L-T groove.
Stages of development of tracheo- esophageal septum during 4th & 5th weeks : • By the end of 4thweek, the laryngotracheal groove evaginated to form pouchlike respiratory diverticulum (lung bud),which is located ventral to the pharynx. • The distal end of diverticulum enlarges to form a globular tracheal bud. • Longitudinal tracheoesophageal folds develop and fuse together to form tracheo-esophageal septum. • This septum divides the foregut into a ventral part,the laryngo-tracheal tube (primordium of larynx,trachea,bronchi & lungs) + a dorsal part (primordium of oropharynx & esophagus).
Stages of development of tracheo-esophageal septum during 4th & 5th weeks : • A,B,&C…. lateral views of caudal part of primordial pharynx showing the respiratory diverticulum and partitioning of foregut by the tracheo-esophageal septum into the esophagus +laryngo-tracheal tube by • D,E,& F… T.S illustrating formation of T-E septum to separate foregut into L-T tube & esophagus.
Development of larynx 4-weeks 5-weeks 6-weeks 10-weeks • The epithelial lining of larynx develops from the endoderm of cranial (upper) end of L-T tube • Laryngeal epithelium proliferates, producing temporary occlusion of laryngeal lumen. • Recanalization of larynx occurs by 10th week, producing a pair of lateral recesses, the laryngealventricles, that are bounded by folds of m.m that forming vocal folds (cords) & vestibular folds. • Laryngeal cartilages (except epiglottis) & ms. develop from the mesenchyme of 4th & 6th pharyngeal arches that is derived from neural crest cells. • This mesenchyme proliferates, producing paired arytenoid swellings, converting the slitlike aperature into T-shaped laryngeal inlet.
Development of larynx • The epiglottis develops from the caudal part of hypopharyngeal eminence which develops from mesenchyme in the venteral ends of 3rd &4th pharyngeal arches, but the cranial part of this eminence forms the posterior (pharyngeal)1/3 of tongue. • Laryngeal ms. develop from mesenchyme of 4th & 6th pairs of pharyngeal arches, therefore they are innervated by laryngeal branches of vagus nerves that supply these arches. • Growth of larynx and epiglottis is rapid during the first 3 years after birth, by this time the epiglottis taking its adult form.
Development of Trachea 4-weeks L-T tube 10 weeks 11 weeks 14 weeks • A, 4-weeks,/ B,10weeks, /C,11weeks….T.Ss of L-T tube, showing that endoderm ofthe lower part of L-T tube gives rise to epithelium (mucosa) & glands of trachea / and that splanchnic mesenchyme surrounding the tube forms C.T, muscle and cartilage. • D, T.S of developing trachea at 14 - weeks.
Development of Bronchi and Lungs : • A,B,C lateral views of caudal part of pharynx during 4th & 5th weeks,illustrating division of tracheal budinto 2 primary bronchial buds at 5th w. • These bronchial buds grow laterally into pericardio-peritoneal canals (primordia of pleural cavities). • Together with the surrounding splanchnic mesenchyme, the bronchialbuds differentiate into the Rt. & left main bronchi and their ramifications in the lungs. 4th week 5th week • A, 5weeks. / B, 6weeks, illustrating growthof the developing lungs into the splanchnicmesenchyme which lies medially to the pericardio-peritoneal canals. /also illustrating development of layers of the pleura at 6th w. 5-weeks 6-weeks
Development of Bronchi and Lungs : • By 5th week the connection of each bronchial bud with the trachea enlarges to form the main bronchus. • The right main bronchus is larger than the left one. • The main bronchi subdivide into secondary bronchi (the right then forms 3 secondary bronchi, and the left2 bronchi) that form lobar, segmental, &intrasegmental branches.
Development of Bronchi and Lungs : • On the right / superior lobar bronchus supplies the upper (superior)lobe of right lung, whereas the inferior lobar bronchus subdivides into 2 bronchi, one to the middle lobe, and the other to the lower (inferior) lobe. • On the left / the 2 lobar bronchi supply the upper & lower lobes of the lung. • Each lobar bronchus undergoes progressive branching.
Development of Bronchi and Lungs : • By the 7th week, The segmental bronchi(10 in the right and 8 or 9 in the left lung), begin to develop. • Each segmental bronchus with its surrounding mass of mesenchyme is the primordium of a broncho-pulmonary segment. • As the lungs develop, they acquire a layer of visceral pleura derived from the splanchnic mesenchyme, and the thoracic body wall becomes lined by alayer ofparietal pleura, derived from the somatic mesoderm.
Maturation of the lungs • Pseudoglandular period (6-16 weeks) • Canalicular period (16-26 weeks). • Terminal saccular period (26 weeks to birth). • Alveolar period (32 weeks to 8 years).
Maturation of the lungs • Pseudoglandular Period : • (6 to 16 weeks) : • All major elements of lung have formed, except those involved with gas exchange. • There are bronchi & terminal bronchioles but, No respiratory bronchioles or alveoli are present. • Respiration is not possible, so fetuses born unable to survive.
Maturation of the lungs Canalicular Period : (16 to 26 weeks) : • Enlagment of lumina of bronchi & terminal bronchioles. • Each terminal bronchiole gives rise to 2 or more respiratory bronchioles, each of which divides into 3 or 6 alveolar ducts. • At the end of this period, respiration is possible due to development of some thin-walled terminal saccules (primordial alveoli) at the end of respiratory bronchioles. • A fetus born at the end of this period maysurvive if given intesive care, but often dies because its respiratory system is still immature.
Maturation of the lungs • Terminal Saccular Period :(26 weeks to Birth) : • Thin-walled many terminal saccules (primitive alveoli) are developed. • Capillaries (endothelial cells) begin to bulge into the epithelium of these primitive alveoli, forming the blood-air barrier, which permits gas exchange for survival of the premature fetus. • The terminal saccules are lined mainly by squamous epithelial cells of endodermal origin-type I alveolar cells or pneumocytes -for gasexchange. • scattered among squamous epithelial cells are rounded secretory epithelial cells-type IIalveolar cells or pneumocytes- which secretepulmonary surfactant (a mixture of phospho-lipids) on the internal walls of terminal saccules, lowering surface tension of alveoli.
Maturation of the lungs • Terminal Saccular Period :(26 weeks to Birth) : • The amount of surfactant increases during the last 2 weeks before birth. • The surfactant begins by 20 weeks but it is present only in small amountsin premature infants (by 26 to 28 weeks), they may suffer from respiratory distress because of surfactant deficiency. • Surfactant counteracts the surface tension forces and facilitates expansionof the terminal saccules (primordial alveoli).
Maturation of the lungs • Alveolar Period : (32 weeks to 8 years) • It is the stage of lung maturation which continues after birth. • Mature alveoli do not develop until after birth,about 95% of alveoli develop postnatally. • The epithelial lining of terminal sacs becomes very thin squamous epithelium. • Type I alveolar cells become so thin that the adjacent capillaries bulge into the terminal saccules • By the late fetal period, the lungs are capable of respiration bescause the alveolo-capillary membrane is sufficiently thin to allow gas exchange, so lungs are capable of functioning as soon as the baby is born.
Maturation of the lungs • Alveolar Period : (32 weeks to 8 years) • Before birth,Breathing movements can be detected by U.S, used in diagnosis of labor. • After birth, increase in the size of lungs results from increse in number of respiratorybronchioles & primordial alveoli rather than from increase in size of alveoli. • As these alveoli increase in size, they become mature alveoli, and the C.T. septa become secondary mature thin septa. • About 50 million alveoli, one –six of adultnumber, are present in lungs of a full-termnewborn infant. • On chest radiographs, lungs of newborn infants are denser than adult lungs. By 8 years, about 300 million alveoli is present.
Maturation of the lungs • Alveolar Period : (32 weeks to 8 years) • At birth, the lungs are half-filled with fluid from amniotic cavity, lungs & tracheal glands. • At birth, This fluid in lungs is cleared by : 1-via mouth & nose by pressure on fetal thorax during delivery. 2- Pulmonary capillaries. 3-Lymphatics & pulmonary arteries & veins. • At birth, lymphatics are more numerous than in adults.
Tracheo-esophageal Fistula • These are the main varities of tracheo-esophageal fistula (TEF). • A,the common type, esophageal atresia(EA) is associated with TEF in more than 85% of cases. • B, fistula between trachea & esophagus. • C, air cannot enter the distal esophagus & stomach. • D, air can enter the distal esophagus & stomach, and esophageal & gastric contents may enter the trachea & lungs.
Tracheo-esophageal Fistula • It is abnormal passage between the trachea & esophagus, males infants are most affected. • It is the most common anomaly of lower respiratory tract, and in more than 85% of cases it is associatedwith esophageal atresia (EA). • It is resulted from incomplete division of the of foregut into respiratory & esophageal parts during 4th week due to incomplete fusion of tracheo-esophageal folds ressults in a defective tracheo-esophageal septum and TEF. • it has 4 types, the most common type is for the superior part of esophagus to end blindly (A). • Polyhydramniosis often associated with esophagealatresia and TEF. This excess amniotic fluid develops because fluid cannot pass to stomach & intestine for absorption and transfering into placenta for disposal. • Gastric contents may reflux via the fistula into trachea & lungs to result in choking and pneumonitis.
The pharyngeal (Branchial) apparatus : • It consists of : 1-pharyngeal arches. 2-pharyngeal pouches. 3-pharyngeal grooves. 4-pharyngeal membranes. • These embryonic structures contribute tothe development of the head & neckregions.
Drawings illustrating the human pharyngeal apparatus. • A, dorsal view of cranial part of an embryo. • B to D,lateral views showing later development of pharyngeal arches. • E to G, ventral or facial views, illustrating the relationship of the firstpharyngeal arch to the stomodeum. -Maxillary prominence of 1st arch lies lateral to stomodeum. -Mandibular prominence of 1st arch lies caudal to stomodeum. • H,horizontal S.of cranial part of emb. • I, horizontal S. illustrating the arch components + floor of pharynx. • J, sagittal S.illustrating the openingsof pharyngeal pouches in the lateral wall of the primordial pharynx.
Pharyngeal arches • They begin to developearly in the 4th week as neural crest cells migrate into the future head & neck regions. • By the end of 4th week,4 pairs ofpharyngeal arches are visible externally • The 5th & 6th arches are rudimentary and not visible on surface of embryo. • Pharyngeal arches are separated externally by fissures- the pharyngealgrooves, which numbered cranio-caudally as the arches. • The arches appear along lateral wall of primordial pharynx. • The primordial mouth (stomodeum) is temporarily closed by oropharyngeal bilaminar membrane (ectoderm & endoderm), which ruptures at about 26days.(during 4th week). Fronto-nasal prominence
Pharyngeal arches • 1st pharyngeal arch (mandibular arch), the primordium of jaws consists of : 1- A dorsal portion, the maxillaryprocess, which gives rise to the maxilla (upper jaw), zygomatic bone, and squamous part of temporal bone. 2- A ventral portion, the mandibularprocess, which gives rise the mandible ( lower jaw). -1st pair of pharyngeal arches plays a major role in facial development. • 2nd pharyngeal arch (hyoid arch) : contributes to the formation of hyoid bone.
Pharyngeal Arches • A, By the end of the 4th week (28days), 4 pairs of pharyngeal arches are developed. • B, Drawing showing pharyngeal pouches + aortic arches, that supplies the pharyngeal arches and arise from truncus arteriosus, then enter the dorsal aorta. The derivatives of aortic arches : are the adult arteries of head & neck. • C, Horizontal section showing the floor of primordial pharynx and germ layerderivatives of the pharyngeal arch components : each arch consists of a core of mesenchyme, which is covered externally by ectoderm and internally by endoderm.
Pharyngeal Arch Components • Each arch consists ofa core ofmesenchyme that is covered externally by ectoderm and internally by endoderm. • A core of mesenchyme derived from the original mesenchyme - mesoderm during 3rd week + neural crest cells (neuroecto-dermal origin) during 4th week that migrate into the arches. • Skeletal musculature & vascular endothelia are derived from the original mesenchyme in the arches. • A typical pharyngeal arch contains :1-an aortic arch artery : arises from truncus arteriosus of primordial heart to enter the dorsal aorta. 2-a cartilaginous rod : that forms the skeleton of arch. 3-a muscular components : to give ms. of head & neck. 4-a nerve : to supply mucosa & ms. of arch.
Fate of Pharyngeal Arches • A, lateral view of embryo at 5th week (32 days) showing pharyngreal arches + cervical sinus. • B, section illustrating growth of 2ndarch over 3rd & 4rth arches. • C, embryo of about 33 days. • D, section illustrating early closureof the cervical sinus during 5th week. • E, embryo of 41 days (end of 6th w.). • F, section showing the transitorycystic remnant of cervical sinus. • G, drawing of 20-week fetus illustrating the area of face derivedfrom the 1st pair of pharyngeal arches.
Fate of Pharyngeal Arches • They contribute to the development of face, nasal cavities, mouth,larynx, pharynx, and neck. • During 5th week, 2nd arch enlarges toovergrow the 3rd & 4th arches, forming ectodermal depression- the cervical sinus. B,D • By the end of 7th week, 2nd to 4th pharyngeal grooves + the cervical sinus have disappeared, giving the smooth contour to the neck
Derivatives of Pharyngeal Arch Cartilages : • A, lateral view of 4-week embryo, illustrating location of cartilages in pharyngeal arches. • B, 24-week fetus illustrating adult dreivatives of arch cartilages :1-Note development of mandible by intramembranous ossification of mesenchymal tissue surrounding the ventral part of 1st arch cartilage (Meckel’s cartilage) + development of malleus & incus (middle ear bones) dorsally + anterior ligament of malleus & sphenomandibular ligament in the middle part.2-Note, the 2nd arch cartilage (hyoid or Reichert’s cartilage) gives rise dorsally stapes & styloid process, in the middle stylohyoid ligament, and ventrally lesser cornu + upper part of body of hyoid bone.
Derivatives of Pharyngeal Arch Cartilages : • B, 3- Note also derivatives of the 3rd arch cartilage which ossifies to form : greater cornu (horn) + inferior part of the body of hyoid bone. 4-Cartilaginous components of 4th & 6th pharyngeal arches fuse to form most of laryngeal cartilages (thyroid + cricoid + arytenoid + corniculate + cuneiform), EXCEPT the cartilage of epiglottis which develops from the mesenchyme of the caudal part of hypopharyngeal eminence lying in the floor of primordial pharynx and derived from 3rd & 4th pharyngeal arches. • The 5th arch is often absent, if present it is rudimentary and has No derivatives.
Derivatives of Pharyngeal Arch Muscles : • A, lateral view of 4-week embryo showing the muscles derived from the pharyngeal arches, the arrow showing the pathway of myoblasts from the occipitalmyotomes to form the muscles of tongue. • B, sketch of head & neck of 20-week fetus, showing the 1st pharyngeal arch forms ms. of mastication & other ms./ 2nd arch forms ms. of facial expression, post.belly of digastric & other ms. / 3rd arch forms stylopharyngeus./ 4th arch forms cricothyroid, levator veli palatini + constrictors of pharynx. / 6th arch forms interinsic ms. of larynx + striated ms of esophagus.
Derivatives of Pharyngeal Arch Nerves • A, lateral view of head &neck and thorax of 4-week embryo showing the cranial nerves :Trigeminal N.(V), Facial N.(VII), Glossopharyngeal N.(IX), and Vagus N.(X)—supplying 1st ,2nd , 3rd & caudal (4th + 6th ) pharyngeal arches, respectively. • B, sketch of head & neck of 20-week fetus showing the 2 branches of 1st arch nerve (CNV), maxillary & mandibular branches of trigeminal N • C, Sagittal section of fetal head & neck showing the sensory nerves of trigeminal N., which isthe principal sensory N. of head & neck supplying face, teeth & m.m. of nasal cavity, palate, mouth & tongue, and is the motor N. for ms. of mastication. • C, The nerves from 2nd to 6th pharyngeal arches have little sensory nerves, however, they innervate m.m. of post.tongue, pharynx & larynx.
Pharyngeal Pouches • The endoderm of the pharynx lines the internal aspects of pharyngeal arches passing into balloonlike diverticula- the pharyngeal pouches. B & C • There are 4 pairs of pouches, the 5th is absent or rudimentary. B & C • The endoderm of pouches contacts the ectoderm of the pharyngeal grooves forming the double-layered pharyngeal membranes separate the pouches from the grooves. C
Pharyngeal Pouches • A,5-weeks embryo, showing that the 2nd pharyngeal arch grows over the 3rd & 4th arches, burying the 2nd to 4th grooves in the cervical sinus. • B,6 -weeks. The endoderm lining the pharyngeal pouches gives rise to important organsin head & neck. • C,7 –weeks. Note migration of the developing thymus,parathyroid, and thyroid glands into the neck.
1st Pharyngeal Pouch • It expands into an elongate tubotympanic recess. • The distal part of this recess contacts the 1st pharyngeal groove to form the tympanicmembrane (eardrum). • The cavity of tubotympanic recess gives rise to tympanic cavity + mastoid antrum. And its connection with the pharynx form pharyngotympanic tube(auditory tube).
2nd Pharyngeal Pouch • The endoderm of 2nd pouch proliferates and grows into the surrounding mesenchyme to form palatine tonsile. • At about 20 weeks (fifth months), the tonsile is infiltrated by lymphatic tissue forming lymphatic nodules of the palatine tonsile. • Part of the cavity of this pouch remains as the tonsillar sinus or fossa.
3rd Pharyngeal Pouch • By the 6th week, the endoderm of 3rd pouch gives rise dorsal part which differentiates into inferior parathyroid gland, and a ventral part which differentiates into the thymus. • Both gland primordia migrate into the neck. Later the parathyroid glands separate from thymus to lie on the dorsal surface of thyroid gland.
Histogenesis of Thymus • Its epithelial tubes and cords are developed from the endoderm of the 3rd pair of pharyngeal pouches, forming the thymic corpuscles. • Its lymphocytes are derived from the hematopoietic cells. • Its mesenchyme and a peculiar ms.cell in the medulla is derived from the neural crest cells. • Growth and development of thymusare notcomplete at birth, but continue until puberty. • At puberty it begins to deminish in size (i.e.,undergoes involution). • By adulthood, it is often scarcely (difficult) recognizable, since it is atrophied and replaced byfatty tissue, however it is still functional for health.
4th Pharyngeal Pouch • By 6th week, the epithelium of the dorsal part of 4th pouch forms the superior parathyroid gland, while of the ventral part forms the ultimopharyngeal body. • The inferior parathyroid glands derived from the 3rdpouch are located inferior to those from 4th one 5th pharyngeal Pouch • If it develops, this rudimentary pouchbecomes part of 4th pouch and contributes to form the ultimopharyngeal body, which fuseswith thyroid gland to give rise to parafollicular cells ofthyroid gland, (C –cells ), which produces calcitonin hormone to regulate the normal calcium level.
Histogenesis of Parathyroid Glands : • The epithelium of the dorsal parts of 3rd & 4th pouchesproliferates during 5th week to form smallnodules on the dorsall aspect of each pouch as the superior & inferior parathyroid glands. • The chief or principle cells are formed during the embryonic period to regulate fetal calcium metabolism. • The oxyphil cells are formed 5 to 7 years after birth (childhood period).
Pharyngeal Grooves • There are 4 pharyngeal grooves (clefts) on each side, that are developed during the 4th & 5th weeks. • These grooves separate the pharyngeal arches externally. • Only one pair of grooves contributes to postnatal structures, the 1st pair groove persists as the external acoustic meatus. • The other grooves lie in a slitlike depression- the cervical sinus. • These grooves normally oblitrated with the sinus as the neck develops.
Pharyngeal membranes • They are formed where the epithelia of the grooves (ectoderm) & the epithelia of pouches (endoderm) approach each other. • Only The 1st pharyngeal membrane gives rise the tympanic membrane (eardrum).
Branchial sinuses : • Branchial sinus :-it is uncommon, it results from failure of 2nd pharyngeal groove & cervical sinus to oblitrate. -it is commonly detected during infancy discharging mucous material. -External branchial sinus : -it opens externally in the inferior part of lateral side of neck along ant.border of sternocliedomastoid ( lateral cervical sinuses). (C,D)-Internal branchial sinus :-Very rare to open internally into pharynx and usually open into tonsillar sinus, resulting from persistence of proximal part of 2nd pharyngeal pouch. (D)
Branchial Fistula, & Cysts : • Branchial fistula : -it results from persistence of parts of2nd pharyngeal groove & pouch. -it passes between the int. & ext. carotid arteries to opens internally into tonsillar sinus and it opens externally into subcutaneous tissue of the lateral side of the neck. (E) • Branchial cyst : -it develops from remnants of thecervical sinus and /or the 2ndpharyngeal groove. -it often lies free in the neck ,just inferior to the angle of mandible. -it may develop along anterior border of sternomastoid or in parathyroid gl. -it is not visible until in late childhood. -it contains fluid & cellular debris of desquamated epithelium. (F)
Branchial Vestige : • It results from cartilaginous or bony remnants of pharyngeal archcartilages appear under skin in the side of neck, Usually anterior to the inferior part of sternocliedo- mastoid ms. (F)
Development of Thyroid Gland : • A, B, & C, sagittal sections of 4, 5, & 6 weeks embryos, illustrating successive stages in the development of thyroid gland. • D, section, showing the path of thyroid gland during its embryonic descend (indicated by the former tract of thyroglossal duct).
Development of Thyroid Gland : • It is the first endocrine gland to develop. • It begins to develop during 4th week (26 days after fertilization) from a median endodermal thickening in the floor of primordial pharynx, which form a small outpouching – thyroid primordium.(A & B) • For a short time the thyroid gland is connected to the tongue by a narrow tube, the thyroglossal duct.(B & C) • The developing thyroid gland descends in the neck, passing ventral to the developing hyoid bone & laryngeal cartilages. (C & D)