Download
1 / 21
210 likes | 224 Views
This study examines the impact of retail clinics on healthcare costs and utilization, using administrative data from a large health insurer. The results suggest that retail clinics serve as lower-cost substitutes for physician visits without negatively affecting the quality of care.

E N D
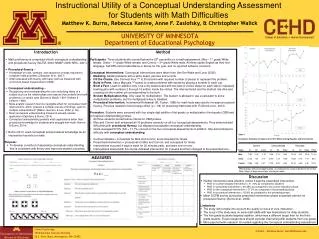
The Impact of Retail Clinics on Cost & Utilization Are They Substitutes or Complements to Physician Services? Stephen T. Parente University of Minnesota Robert Town University of Minnesota and NBER Presentation at International Health Economics Association Meeting July 15, 2009
Rationale for Investigation • Retail Clinics emerged as a health market innovation in 2000. • In general, innovation is welfare enhancing whether it is through new products or through reorganization of products and services. • A concern is that these organizations can exploit administrative pricing irregularities and knowledge gaps of consumers leading to reductions in consumer welfare. • Advocates of retail clinics argue they improve the efficiency of a highly inefficient health care delivery system. • Critics of retail clinics complain that the new service only adds to the inefficiency in the system and could greatly reduce consumer well being from a clinical perspectives.
Summary of Investigation • Objective: Examine the impact of retail clinics on cost and use. • Data: Administrative data from a large health insurer across multiple US markets to examine the evidence of the effects of retail clinics. • Study design: Pre and post retail clinic launch differences in utilization between a treatment population of retail clinic users and retail clinic non-users. • Econometrics: OLS and IV estimation on cost and utilization measures. • Results: We find evidence that retail clinics are lower cost substitutes for physician office visits and their subsequent use does not appear to adversely affect measurable proxy metrics for quality of care. • Implications: The introduction of retail clinics appears to be welfare enhancing.
Prior Commentary & Literature • Rosenblatt, et al, 2006: Concerns of retail clinics taking away business from Community Health Centers. • Kamerow, 2007: Title says it all: “Retail Health Clinics – Threat or Promise?” British Medical Journal • Mehrotra et al, 2008: Used ambulatory care survey information to show the most common conditions seen be those going to retail clinics. Provided a descriptive analysis of differences in physician service use and cost between retail and non-retail clinic users. • No previous direct empirical analysis of total cost, use or welfare impact of retail clinics.
Data • Administrative insurance claims data • Date of service, zip code of provider of care and insured, allowed charge • Diagnosis and procedure code (CPT) • Medical, institutional and pharmacy claims • Used claims available for calendar year 2004 through 2006 • Provider contract data • Retail clinics operating by site of actual clinic (as opposed to corporate headquarters). • Address of actual clinic served • Start date of clinic contract • Unit of Analysis • Cost & Use measures within 180 day intervals indexed on start date of retail clinic opening and they get a retail clinic CPT. One pre-interval and four-post intervals.
Study Population • Retail Clinic Users (Treatment Population) • Need to use at least one retail clinic service • Starting N = 31,392 • Enrolled for one year and had pre clinic launch health care use 6 month prior to launch N = 23,227 • Non-Retail Clinic Users (Control Population) • Population who lived in area when clinic was operating • Population who lives in area when clinic was about to open • Need to use at least one CPT that was used in by a retail clinic • Random sampled from a large N to get at starting N = 39,111 • Enrolled for one year and had pre clinic launch health care use 6 month prior to launch N = 27,008
Patient Case-mix measured using ADGs • Adjusted Diagnostic Groups (ACGs) were developed by Johns Hopkins University • Based on combination of diagnosis, age, gender information during a period of time • Can explain variation in cost as well as risk-adjustment for premium calculation
Top 10 Conditions Seen at Retail Clinics Very similar results to Mehrotraet al, 2008
Demographics of Retail Clinic and Non-Retail Clinic User Populations – 1 of 3
Demographics of Retail Clinic and Non-Retail Clinic User Populations – 2 of 3
Demographics of Retail Clinic and Non-Retail Clinic User Populations – 3 of 3
Empirical Framework • To assess the impact of retail clinic utilization on the expenditures and the patterns of care for enrollee iin market m in period t we estimate parameters from the following model: • yimt= am + x’itb +rrit + eimt • where yimtis one of several different measures of expenditures or utilization. • am is a market fixed effect, xitis a vector of individual demographic, condition and severity controls. • ritis an indicator for whether the enrollee visited a retail clinic and • eimtis a mean zero residual. • The parameter of primary interest is r which captures the impact of retail clinic utilization on the outcome of interest.
Endogeneity issue • Endogeneity of the decision to use a retail clinic. • We address this concern using an instrumental variable approach. • Instrument is the distance from the patient’s home zip code to the nearest retail clinic in operation. If there is no clinic open within 50-miles the distance variable is set to 50 miles. Use instrument^2 as well. • Gowrisankaran and Town (1999), Geweke, Gowrisankaran and Town (2003), and McNeil, McClellan & Newhouse (1994) use a similar identification strategy to measure hospital quality.
Core findings • Costs are less in general for retail clinics • Most of the cost savings is due to reduced physician allowed claim cost • Substantial reductions in admissions and outpatient hosts for chronically ill. • Substantial reduction in ER use and cost for pediatric population. • Results hold in IV estimation. Priviledged & Confidential, HSI Network LLC
Limitations & Extensions • One insurer’s data. But data is internally consistent by person. • Additional instruments. But distance is not a bad way to go for now. • Retail clinic population needs to be weighted to correct for over-sampling general population. Question is, what is the right weight?
Next Potential Steps Beyond Scope • Use clinical metrics for evidence-based medicine as dependent variables. • Drug compliance requires a refill and days supplied variable and also requires a lot of caveats. • But, we don’t find pharma is really in play, but it could change with more precise measures. • At the very least, if no pharma change – the cost reductions for the chronically ill do not pose a quality concern.
Conclusions • Patients who visit retail clinics have fewer costs without any reduction in our admittedly crude measures of quality • Results suggest retail clinics are serving as substitutes for medical care with no obvious quality concerns • More investigation is needed as this market evolves