Download
1 / 36
360 likes | 474 Views
The land of chronic Lyme. Everything works sometimes Eric Gordon MD gordonmd@gordonmedical.com. Does chronic Lyme exist. Multiple animal models demonstrating borrelia despite previous antibiotic therapy

E N D
The land of chronic Lyme Everything works sometimes Eric Gordon MD gordonmd@gordonmedical.com
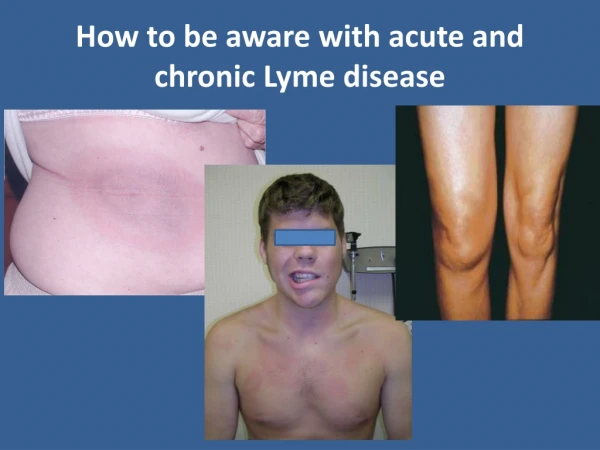
Does chronic Lyme exist • Multiple animal models demonstrating borrelia despite previous antibiotic therapy • We see persistent IgM antibodies with and without IgG antibodies in patients with symptoms that revert to negative IgM status with antibiotic treatment and symptom resolution • Multiple studies demonstrating borrelia persistence in humans despite antibiotic therapy • Our experience of positive Lyme cultures after prolonged antibiotic therapy
Then why does IDSA insist that it doesn’t • Lyme culture was not commercially available and it is an extremely fastidious organism • Patients have multiple complaints that provoke the “psychological reflex” in physicians • Other than a tendency to low wbc counts patients have normal labs ordered by most doctors including sed rate and Crp
Then why does IDSA insist that it doesn’t • Several studies showing no “significant “ improvement with repeated 1-2 month courses of antibiotics • Fallon study showing minimal improvement with 6 months of rocephin (ceftriaxone) • Stridency of patients with unexplained chronic complex symptoms and normal tests and “normal” PE who are referred to Infectious disease specialists by doctors and family
Problem of standard Western Blot testing • Chronic patients often have negative IgG Western Blots (WB) and “false “ positive IgM WB • Labcorp and Quest WB’s have low sensitivity and are especially poor outside of new England • We don' t know the number of people who have Lyme who have a failure to develop antibodies
Problem of standard Western Blot testing • WB testing bands Decided at conference held by CDC in Dearborn , Michigan in 1994. The IgG criteria were based on a paper from 1993 by Dressler, Whalen, Reinhardt and Steere . They looked at WB's from several dozen well characterized Lyme patients with strong immune responses and found that by requiring 5 out of 10 IgG bands the WB could be highly specific but did lose some sensitivity
Problem of standard Western Blot testing • IgM criteria were developed from other similar papers only 2 of 3 IgMbands are necessary . The first IgM bands that show up are 41, 22-25 , and 39.41 is to the flagellar protein and is not specific to LymeThe CDC has decided that since IgM is an acute event you should ignore it starting 6 weeks after infection
Problem of standard Western Blot testing • Early sub-therapeutic treatment can interfere with the immune response leading to negative antibody tests • Many people who relapse after antibiotic treatment are sero-negative till after retreatment • Some people with culture positive Lyme disease are sero negative by WB even though they were positive when first diagnosed years earlier • Sometimes they are sero-negative because all the antibody is tied up in immune complexes
Lyme specific bands according to ILADS and our clinical judgment • 31= OspA 22-25 = OspC 34= OspB 18, 39, 83-94CDC criteria leave out 31 and 34 even though they are specific for Lyme disease because they tend to show up later in the disease and this wasn't the population Dressler et al studied.31 is OspA which is the antigen used in the early Lyme vaccines ( Osp=Outer surface protein)
Everybody is right but nobody trusts each other • Chronic Lyme exists and sometimes antibiotics help • People develop autoimmune diseases and sometimes removing the trigger helps(Lyme ) • IDSA studies only include patients who fit CDC criteria-circular reasoning • Sometimes antibiotics don’t help and make people worse • Unneeded antibiotics cause severe dysbiosis • PICC line infections do happen
Testing limitations and controversies Advanced laboratory Systems (ALS) • Need to be off all treatment for 4 weeks and best to draw in afternoon when symptomatic • Initial darkfield exam then 10-14 day culture and repeat darkfield if negative another 8 week and if needed another 8 weeks of culture • If positive darkfield then borrelia specific staining and if desired PCR for species • 100% negatives on controls • 7% false negatives in patients • B Garini found in high % of cultures done in Sapi lab leading to claims of contamination. This is not same location as ALS lab.
Testing limitations and controversies iSpot • Melisa test evaluating T cell reactivity measuring Interferon gamma production after exposure to Lyme antigens • Main problem is lots of false negatives but at least they identify them • Because in chronic patients there is high percentage of poor T cell Interferon gamma production after stimulation by phytohemagglutinin as a screening test • Pharmasan.com
Testing limitations and controversiesprovoked urine testing • IDSA –unproven • Requires oral or IM antibiotic provocation • Measures Lyme antigen in urine • Igenex .com
Testing limitations and controversiesDNA PCR testing • IDSA –unproven • DNA may remain but non-viable and non-infectious • Milford Medical lab Borreliaburgdorferi, and Borreliamiyamotoi • Igenex lab
Complicating issues • Mold and other neurotoxins • Co-infections • Biochemical individuality (genetics and epigenetics) • Dysbiosis • Heavy metals • EMF • Psyche • Structural • Dental • Biofilms
Mold Always suspect when you think babesia and especially when pain and brain fog are out of proportion and especially when intermittent • Realtime lab mycotoxin panel $700 initial followup $200 • Best to collect urine in the AM after sauna or several days of Glutathione • Dr Brewer uses CSM but also charcoal and bentonite for tricothecene and aflatoxinToxins 2014, 6, 66-80; doi:10.3390/toxins6010066
Mold • Dr Shoemaker –Visual Contrast Study for neurotoxicity, markers of innate immunity C4a, VIP ,MSH, VEGF. TGF-beta-1, CD4CD25++, • Remove from exposure and use binders then nasal VIP when other markers are corrected • He prefers Cholestyramine (CSM) • Please see Dr Shoemakers website Survivingmold.com
Neurotoxins • Mold, Babesia, Lyme • Lipophyllic-use intestinal binders • Cholestyramine, welchol, chitosan, charcoal, bentonite, zeolite • Start slow – moving toxins can cause symptoms • Remove from exposure
Co-infections • Bartonella, Babesia, Ehrlichia • Protomyxomarheumatica ? • Mycoplasma pneumonia • Chlamydia Pneumonia • Rickettsia’s • Tularemia, Q fever (CoxiellaBurnetii) • Parasites • Viruses-EBV, HHV6,CMV, Coxsackie
Parasites • If any clinical hint, treat parasites first, and repeatedly, if any clinical response. • Multiple herbal treatments • Biltricide for flukes, tapeworms • Ivermectin for microfilaria • Pyrantelpamoate for hookworms and roundworms • Albendazole- roundworms, tapeworms and flukes • Alinia- for everything -caution
Biochemical individualityepigenetics and genetics • Methylation cycle- MTHFR Ben Lynch et al, Glutathione –Von Konynberg ,Nathan –order phenotype testing from Vitamindiagnostics.com • HLA-DR per Ritchie Shoemaker 04-3-53 and 11-5-51 etc some correlation with sicker patients- defects in antibody presentation or toxin problems
Biochemical individualityepigenetics and genetics • Celiac and gluten sensitivity • Porphyria- spot urine when symptomatic • Kryptopyrroluria • Mast cell activation • Cytochrome p450 variations • Oxalate –Susan Owens lowoxalates.com
Heavy Metals • Mercury , Lead, Arsenic, Cadmium • Aluminum • Hair analysis • Quicksilver –hair, serum, and urine • DMPS, CaEDTA challenge test- make sure glutathione is adequate and patient not too toxic • DMSA
EMF • Check house and work • Remove toxins and strengthen membrane integrity • Decrease inflammation • Richard Conrad—ConradBiologic.com • Stetzerelectric.com
Psyche • Not psychological • Bugs effect nervous system • Amplification of your normal neurotic qualities • Sensitization to all input • Loss of social support • Therapy that the patient can receive - have different modalities • Annie Hopper , Ashok Gupta, others
Structural issues and Detox • Inflammation + structural dysfunction = pain and a good place for bugs and toxins to accumulate • Need osteopath, chiropractor, physical therapist, massage therapist • Acupuncture, FSM (frequency specific microcurrent) Scenar, laser, ,photon stim etc. • Sauna, colonics, baths • Rectal ozone • Diet, diet, nutrition, diet, trace minerals ,diet
Dental • Chronic infections-wisdom teeth sites, root canals • Need ICAT –plain films will miss infection • TMJ • Mercury • Galvanic testing when metal is present
Biofilms • planktonic forms are where we look for the bugs but it but they live in biofilms • Complex structures-hi in Ca,Mg, Fe • Don’t try to destroy them too early • EDTA, Enzymes, Silver • Costerton, J. W youtube.com/watch?v=M_DWNFFgHbE
Bottom line • Listen and look closely at your patient • If robust and recent onset of symptoms feel free to use antibiotics but consider herbal treatments first if you feel infection has been there for more than 6-12 months. Less antibiotics the better. • Sensitive and sick for a long time- start slow and don’t think you can’t mess them up with energetic or herbal therapies
Treatment • Always use probiotics and saccharomycesboulardi • Join ILADS and read Burrascano and Horowitz • Do an ILADS preceptorship • Start slow and believe your patients
TreatmentsAntibiotics • Oral –Hi dose Doxycycline and rifampin with macrolides and hydrochloroquine • Omnicef 300mg two bid with macrolides • Bactrim DS bid with rifampin 300mg bid +/- macrolides or just rifampin 300mg bid +/- macrolides • Macrolides-Zithromax 250-600mg and Biaxin 1000mg qd usually with hydrochloroquine • All of these can and should be modified to patient tolerance especially rifampin (cytP450 issues) Use Biaxin instead of Zithromax with rifampin • Metronidizole, Tindamax (cyst busters)
TreatmentIV antibiotics 3days out of 7 Standard therapy Rocephin 2 gm bid remember to add Actigal 300mg bid My preference is Claforan 4 gm tid Many other options best to discuss with experienced clinicians Occasionally if no response to cephalosporinsVancomycin 1 gm q12 hours with trough levels between 10-20 is effective (Bartonella) I almost always add Argentyn 23, 30cc per day for its synergistic effect Pulse therapy and consider Doxy , macrolides , Rifampin, Tinidizole, and be extra cautious with quinolones
Other IV therapies • Ozone Dr David Minkoff and also hi pressure ozone per Dr Robert Rowan and Dr Woitzel , Zotzmann in Germany makes a machine • H2O2 2.5-5cc of 3% with 10cc DMSO in 250-500cc D5W with Mn and MgCl to protect veins per Dr Brodie • UVB treatments • IV homeopathics to help detox • IV silver to augment antibiotics • IV Phosphatidylcholine ,phenylbutyrate and glutathione for detox
TreatmentBasic Herbal list • Nutramedix---Samento, Banderol, Cumanda, Enula • Classical Pearls- Lightening and Thunder pearls • Dr Zhang- HH • Byron White –A-L, A-Bart , A-Bab, A-Myco • Beyond balance BB-1, Bab-1&2, Bart-1 • Dr Buhner- Japanese knotwood, cats claw, sidaacuta, cryptolepsis
Immune Support • GcMAF -measure Nagalase at health diagnostics- oral and injectable forms • Vit D – check 25 and 1-25 Vit D • LDN –low dose naltrexone • Herbs
Energetic treatments • Multiple Vega and subsequent devices for diagnosis and treatment • Frequency generating machines such as Doug coil, pulsedtechnologies.com, many others • Biophoton therapies –Dr Woitzel in Germany and Johan Boswinkel in Netherlands