Download
1 / 1
10 likes | 192 Views
The Value of NT-proBNP for the Evaluation of Acute CHF: A Multi-center, International Pooled Analysis of 1256 Subjects: Primary Results from the I nternational C ollaborative o f N T-proBNP (ICON) Study

E N D
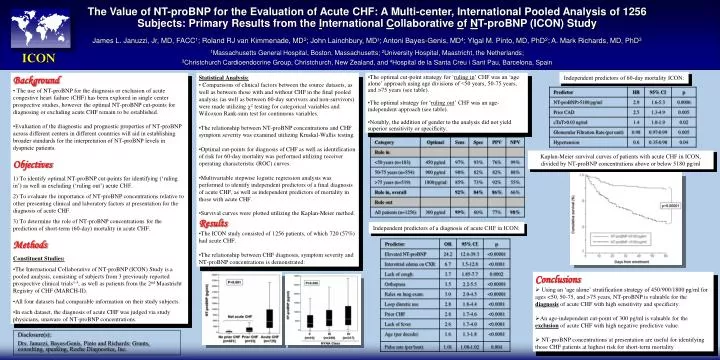
The Value of NT-proBNP for the Evaluation of Acute CHF: A Multi-center, International Pooled Analysis of 1256 Subjects: Primary Results from the International Collaborative of NT-proBNP (ICON) Study James L. Januzzi, Jr, MD, FACC1; Roland RJ van Kimmenade, MD2; John Lainchbury, MD3; Antoni Bayes-Genis, MD4; YIgal M. Pinto, MD, PhD2; A. Mark Richards, MD, PhD3 1Massachusetts General Hospital, Boston, Massachusetts; 2University Hospital, Maastricht, the Netherlands; 3Christchurch Cardioendocrine Group, Christchurch, New Zealand, and 4Hospital de la Santa Creu i Sant Pau, Barcelona, Spain ICON Independent predictors of 60-day mortality ICON: • Background • The use of NT-proBNP for the diagnosis or exclusion of acute congestive heart failure (CHF) has been explored in single center prospective studies, however the optimal NT-proBNP cut-points for diagnosing or excluding acute CHF remain to be established. • Evaluation of the diagnostic and prognostic properties of NT-proBNP across different centers in different countries will aid in establishing broader standards for the interpretation of NT-proBNP levels in dyspneic patients. • Objectives 1) To identify optimal NT-proBNP cut-points for identifying (‘ruling in’) as well as excluding (‘ruling out’) acute CHF. 2) To evaluate the importance of NT-proBNP concentrations relative to other presenting clinical and laboratory factors at presentation for the diagnosis of acute CHF. 3) To determine the role of NT-proBNP concentrations for the prediction of short-term (60-day) mortality in acute CHF. Methods • Constituent Studies: • The International Collaborative of NT-proBNP (ICON) Study is a pooled analysis, consisting of subjects from 3 previously reported prospective clinical trials1-3, as well as patients from the 2nd Maastricht Registry of CHF (MARCH-II). • All four datasets had comparable information on their study subjects. • In each dataset, the diagnosis of acute CHF was judged via study physicians, unaware of NT-proBNP concentrations. • Statistical Analysis: • Comparisons of clinical factors between the source datasets, as well as between those with and without CHF in the final pooled analysis (as well as between 60-day survivors and non-survivors) were made utilizing 2 testing for categorical variables and Wilcoxon Rank-sum test for continuous variables. • The relationship between NT-proBNP concentrations and CHF symptom severity was examined utilizing Kruskal-Wallis testing. • Optimal cut-points for diagnosis of CHF as well as identification of risk for 60-day mortality was performed utilizing receiver operating characteristic (ROC) curves. • Multivariable stepwise logistic regression analysis was performed to identify independent predictors of a final diagnosis of acute CHF, as well as independent predictors of mortality in those with acute CHF. • Survival curves were plotted utilizing the Kaplan-Meier method. • Results • The ICON study consisted of 1256 patients, of which 720 (57%) had acute CHF. • The relationship between CHF diagnosis, symptom severity and NT-proBNP concentrations is demonstrated: • The optimal cut-point strategy for ‘ruling in’ CHF was an ‘age alone’ approach using age divisions of <50 years, 50-75 years, and >75 years (see table). • The optimal strategy for ‘ruling out’ CHF was an age-independent approach (see table). • Notably, the addition of gender to the analysis did not yield superior sensitivity or specificity. Kaplan-Meier survival curves of patients with acute CHF in ICON, divided by NT-proBNP concentrations above or below 5180 pg/ml Independent predictors of a diagnosis of acute CHF in ICON: • Conclusions • Using an ‘age alone’ stratification strategy of 450/900/1800 pg/ml for ages <50, 50-75, and >75 years, NT-proBNP is valuable for the diagnosis of acute CHF with high sensitivity and specificity. • An age-independent cut-point of 300 pg/ml is valuable for the exclusion of acute CHF with high negative predictive value. • NT-proBNP concentrations at presentation are useful for identifying those CHF patients at highest risk for short-term mortality Disclosure(s): Drs. Januzzi, Bayes-Genis, Pinto and Richards: Grants, consulting, speaking, Roche Diagnostics, Inc.






















