Download
1 / 55
550 likes | 584 Views
Explore the pathophysiology and clinical aspects of goiter, including iodine intake, genetic factors, and related conditions like Cretinism and Thyroid Hormone Synthesis. Learn about goiter development, mutations, treatment, and more.

E N D
Goiter: Pathophysiology and clinical aspects Joaquín Lado Abeal, MD, PhD Department of Internal Medicine TTUHSC-SOM, Lubbock
Iodine intake (goitrogens) Gender Genetic
From Iodine Satus Worldwide. WHO Global Data Base on Iodine Deficiency. 2004
From Iodine Satus Worldwide. WHO Global Data Base on Iodine Deficiency. 2004
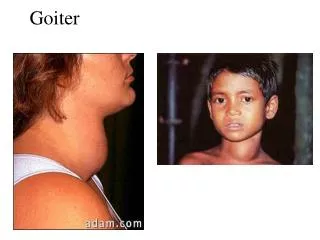
CRETINISM Myxedematose Neurological
TSH Hyperthyrodism Hypothyrodism T4 T3 High T4/T3 Low TSH Low T4/T3 High TSH
Insulin/IGF-I TSH Diferentiation Proliferation
Pituitary TSHoma TSH
0 100 200 300 400 500 600 51 49 47 45 250 15 200 150 10 100 5 50 0 0 250 200 150 0 100 200 300 400 500 600 Syndrome of Resistance to Thyroid Hormone Action (SRTH) 37 36 Neck diameter (cm) 35 34 Weight (Kg) 33 32 31 30 November 2001 2 1 0.5 TSH (mU/L) (µg/L) TT4 (µg/dl) TG 0.1 0. 05 L-T dose 3 µg c.2.d. Number of days May 2003
TSH (µU/ml) MA Pisarev, RD Utiger, JP Salvaneschi, N Altschuler, LJ DeGroot. Serum TSH and thyroxine in Goitrous Subjects in Argentina. J Clin Endocr. 30:680-681. 1970.
MULTINODULAR GOITER 28.1.04 30.8.05 NORMAL 11.4.05 TSH µU/ml 0.08 0.35-5.50 0.42 0.10 1.08 FT4 ng/dl 0.88 0.80 0.85-1.86 3.65 3.29 3.89 2.20-4.70 FT3 pg/ml Ab TPO < 33 AbTG < 100
Total Thyroidectomy (February 05) 50 µg/day T4 (starting March 04) 100 µg/day T4 Post surgery (starting February 05) 100 µg/day T4 (starting Nov 04)
rT3 D3 T3 MCT8 T4 T4 T3 D1, D2 T4
T wildtype GTAAGTTCATTG mutant TAAGTTCATTG c.886C>T p.R277X c.6205+1delG Exon 35 skipping THYROGLOBULIN GENE MUTATIONS Red=goiter R277X c.6205+1delG WT/ c.6205+1delG WT/ c.6205+1delG WT/ c.6205+1delG WT / WT WT/ p.R277X p.R277X / c.6205+1delG p.R277X / c.6205+1delG p.R277X / c.6205+1delG p.R277X / c.6205+1delG T Intron 35 Exon 35 Exon 7
Exon 35 skipping TT GCT CAA AAT AAT GCT CCC AGT TTT TGC CCT TTG GTT GTT CTG CCT TCC CTC ACA GAG AAG I A Q N N A P S F C P L V V L P S L T E K K P M S L Exon 36 Exon 34
WT /c.6205+1delG p.R277X /c.6205+1delG
Thyroglobulin mutations unfolded protein response apoptosis defective hormone synthesis p53, NF-kB, MPAKs, VEGF high serum TSH Goiter oxidative stress BRAF mutations Cancer
Afrikaner cow 9 TG 48 1
RAS INACTIVE Pi GEF GDP GTP GAP GTP GDP ACTIVE
PLC DAG PKC R Wetzker, Frank-D Bohmer. Transactivation joins multiple tracks to the ERK/MAPK Cascade. Nature Reviews. Molecular Biology. 4: 651-657. 2003.
GTP RAS RalGDS Raf PLC PI3K MEK Ca 2+ intracelular AKT/PKB Ral ERK Growth, cell survival H2O2 H2O2 Transcription Proliferation Cell survival Proliferation
RAS Mutations in Thyroid Tumors 30% Colloid nodules 25% Follicular adenomas Papilary carcinomas 20% Follicular carcinomas 15% 10% 5% 0% H1-RAS (12/13) H2-RAS (61) K1-RAS (12/13) K2-RAS (61) N1-RAS (12/13) N2-RAS (61) V. Vasko et al. JCEM. 88(6):2745-2752. 2003
Normal Human Thyrocites TTF-1 PAX-8 Tg 3 Weeks 3 Weeks 4 Days CONTROL H-RAS (V-12) V Gire, D Wynford-Thomas. Oncogene. 19:737-744.2000
RAS RalGEF PI3K MAPK CELL SURVIVAL PROLIFERATION GROWTH
Chromosomal imbalance t(2;3)(q13;p25) & -20 15q loss AR Marques et al. JCEM. 87(8): 3947-3952. 2002
PAX8-PPARG t(2;3)(q13;p25) TG Kroll et al. Science. 289:1357-1360. 2000 Placzkowski KA et al. PPAR Research. 2008
A PPARg 1 (exon 1) PAX8 (exon 8) B PPARg 1 (exon 1) PAX8 (exon 10) PAX8 (exon 10) PAX8 (exon 8)
Chernobyl Disaster (April 26 1986)
Aneuploidy (33% Goiters) 66 XXX From T Dettori et al. Genes, Chromosomes & Cancer. 38: 22-31. 2003.
M Iliszko et al. Cancer Genetic and Cytogenetcis. 161: 178-180. 2005