Download
1 / 30
360 likes | 1.46k Views
Goiter. Dr. Gehan Mohamed. Thyroid enlargement. The term goiter (from the Latin guttur = the throat) is used to describe generalised enlargement of the thyroid gland. NORMAL SIZED THYROID (black lining). ENLARGED GOITER (pink). Causes of Goiter. GOITER.

E N D
Goiter Dr. Gehan Mohamed
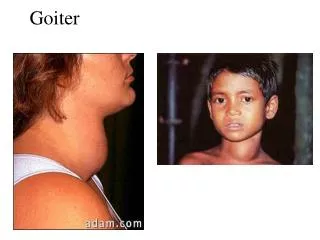
Thyroid enlargement • The term goiter (from the Latin guttur = the throat) is used to describe generalised enlargement of the thyroid gland.
NORMAL SIZED THYROID (black lining) ENLARGED GOITER (pink)
GOITER A goitre may be associated with: Normal thyroid hormonal activity (euthyroidism). Increased thyroid hormonal activity (hyperthyroidism). Decreased or absent thyroid hormonal activity (hypothyroidism).
Classification of Goiter • Simple (non-toxic ) Goiter a- Diffuse goitre b-Nodular goitre Either diffuse or nodular goiter can be sporadic or endemic when more than 10% of any community have goiter . • Toxic Goitre a- Diffuse toxic goiter(Grave’s Disease) b- nodularToxicgoiter
Hypothalamus TRH Anterior pituitary TSH Thyroid T4 Remember this? Iodide T3
io Simple Goiter Definition :it is goiter with normal thyroid hormonal functions. Age group: May occur in any age group-from neonate (congenital goiter) to the elderly. Peak age:31 and 40 years. The goiter appears in childhood in endemic areas but, in sporadic cases, it usually occurs at puberty when metabolic demands are high.
Aetiology of goiter • A- deficiency of the thyroid hormones lead to Increased secretion of TSH which stimulate thyroid to grow: causes of thyroxine deficiency are: • Inadequate iodine in diet • Impaired absorption of iodine from the gut • Drugs preventing trapping and concentrating of iodine by the thyroid gland • Dyshormonogenesis: deficiency of enzymes necessary for oxidising iodine, coupling of iodine and tyrosine • Excessive iodine paradoxically interfering with release of hormones from the thyroid. • Goitrogens: Well-known goitrogens as cabbage,cauliflower,turnip which contain thiocyanate which prevent thyroxine hormone production.
Aetiology of goiter B- inappropriate secretion of TSH from a microadenoma in the anterior pituitary C- Relative Physiological Deficiency: Physiological states such as puberty ,menstruation, pregnancy and lactation there is Increase demand for thyroid hormones due to increase in metabolic activity
Mechanism of enlargment of thyroid in case of Simple Goiter: The stages in goiter formation are as follows: •1- decrease level of thyroxine hormone secretion stimulate release of excess TSH which cause growth stimulation and diffuse hyperplasia of the thyroid gland ; all lobules are composed of active follicles and iodine uptake is uniform. This is a diffuse hyperplastic goiter, which may persist for a long time but is reversible if stimulation ceases. • 2- Later, as a result of fluctuating stimulation of the thyroid (alternating hyperplasia and involution of the thyroid ), a mixed pattern develops with areas of active lobules and areas of inactive lobules. • Active lobules become more vascular and hyperplastic until haemorrhage occurs, causing central necrosis and leaving only a surrounding rind of active follicles. • Necrotic lobules coalesce to form nodules filled with either iodine-free colloid or a mass of new but inactive follicles. • Continual repetition of this process results in a nodular goitre. Most nodules are inactive, and active follicles are present only in the inter nodular tissue
Diagnosis of simple goiter Symptom: swelling in the neck-a major complaint .Pressure symptoms like difficulty in swallowing and breathing . Examination findings on Nodular Goitre • A visible goiter that moves up and down on swallowing • May be small, moderate, large or giant in size and affects one of the two lateral lobes or the isthmus or all the lobes. • Skin over goiter is often shiny with engorged superficial veins . Investigations • Imaging: x-ray of the neck including thoracic inlet,, ultrasound, CT scan • Thyroid function test • Direct and indirect laryngoscopy
COMPLICATIONS OF simple GOITER • Pressure symptoms-dyspnea, dysphagia • Toxicity-secondary thyrotoxicosis may occur • Malignant change • Infection
ectomy Management of simple goitre Prevention • Iodine supplementation in food Drug Therapy • Iodine therapy-Lugol’s iodine or potassium iodide tablets-early cases of endemic and sporadic goitres especially adolescent hyper plastic goitre • Thyroxine and its analogues-diffuse hyperplastic goitre. Surgery :thyroidectomy for simple nodular goitre Indicated for the following reasons: • An increasing growing thyroid • Trachea compression • May become toxic • Malignancy may occur
2- Toxic goiter Types of Toxic goiter: 1- Graves’ disease (primary toxic goiter ): a diffuse goiter associated with hyperthyroidism. Age group : usually occurs in younger women and is frequently associated with eye signs. 50% of patients have a family history of autoimmune endocrine diseases. • Mechanism : Graves disease is an autoimmune disease that cause hypertrophy and hyperplasia of the thyroid due to abnormal thyroid-stimulating antibodies (TSH-RAbs) that bind to TSH receptor sites and produce a disproportionate and prolonged effect. • Triad of Graves disease: 1- hyperthyroidism 2- exophthalmos due to deposition of proteoglycans ,edema,lymphocytic infiltrate. 3 – dermopathy in form of pretibial myxedema
Toxic goiter 2- Toxic nodular goiter (secondary thyrotoxicosis): A simple nodular goiter is present for a long time before the hyperthyroidism, usually in the middle-aged or elderly, and is very infrequently associated with eye signs.
Diagnosis of toxic goiter • A- manifestations due to enlargment of the thyroid • Swollen front of the neck • A tight feeling in the throat • Coughing • Difficulty in swallowing & breathing
Symptoms: Hyperactivity Irritability Heat intolerance & sweating Palpitations Fatigue & weakness Weight loss with increased appetite Diarrhea Polyuria Sexual dysfunction Signs: Tachycardia Atrial fibrillation Tremor Goiter Warm, moist skin Muscle weakness, myopathy Lid retraction or lag Gynecomastia * Exophtalmus * Pretibial myxedema B- manifestations of THYROTOXICOSIS
Graves’ disease :Diffusely enlarged gland , Can weigh up to 200 g ,Richly vascular
colloid Thyroid epithelial cells T4 90% T3 10% Normal Thyroid TSH
Toxic goiter:scalloping of colloid inside thyroid folliclessmall sized follicles , lymphocytic infiltration,hypervascularity
Thyrotoxicosis - differential • Graves’disease • Toxic adenoma (solitary) • Toxic multinodular goiter • Subacute thyroiditis • Hashimoto’s thyroiditis (transient hyperthyroid phase) • Thyrotoxicosis factitia • Postpartum • Struma ovarii • Metastatic thyroid carcinoma • Hydatidaform mole • TSH-secreting pituitary tumor • Pituitary resistance to triiodothryonine and thyroxine
Other clinical presentations for patients with goiter • As we previously mentioned patients with goiter may be : 1- euthyroid : normal thyroid functions 2- hyperthyroidism :toxic goiter 3- hypothyroidism: decrease thyroid functions , - hypothyroidism In infants called cretinism - hypothyroidism In adults called myxedema
Symptoms: Tiredness Weakness Dry skin Sexual dysfunction Dry skin Hair loss Difficulty concentrating Signs: Bradycardia Dry coarse skin Puffy face, hands and feet Diffuse alopecia Peripheral edema Delayed tendon reflex relaxation Carpal tunel syndrome Serous cavity effusions. HYPOTHYROIDISM