Download
1 / 31
400 likes | 1.12k Views
CELL WALL SYNTHESIS INHIBITORS . CELL WALL SYN. INHIBITORS. BETA LACTAM ANTI BIOTICS PENCILLINS CEPHALOSPORINS CARBAPENEMS MONOBACTAMS. Beta- Lactam Antibiotics. Beta- Lactam Antibiotics. Strep throat IM, syphilis. Skin infections fm staph/strep. Bacterial URI.

E N D
CELL WALL SYN. INHIBITORS • BETA LACTAM ANTI BIOTICS • PENCILLINS • CEPHALOSPORINS • CARBAPENEMS • MONOBACTAMS
Beta- Lactam Antibiotics Strep throat IM, syphilis Skin infections fm staph/strep Bacterial URI SE: Hypersensitivity is primary problem. Pruritic rash. Anaphylaxis also occurs.
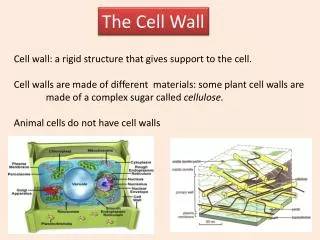
Penicillins • Bactericidal • Peptidoglycan cell wall organisms • Not effective against Mycobacterium, Protozoa , Fungi & viruses.
Interfere with last step of bacterial synthesis—trans peptidation • Results in exposure of less stable membrane. • Cell lysis occurs through osmotic pressure or activation of autolysins • Thus they are bactericidal.
Penicillin binding proteins • Penicillins inactivate many proteins on the bacterial cell membrane. These pbps are bacterial enzymes involved in the synthesis of the cell wall • Inhibition of trans peptidase • Production of autolysins
Antistaphylococcal penicillins • All are stable to penicillinase • Cloxacillin • Dicloxacillin • Methicillin • Nafcillin • Oxacillin
Antipseudomonal penicillins • Particularly active against P. aeruginosa • Azlocillin • Carbenicillin • Mezlocillin • Piperacillin • Ticarcillin
Clinical use of penicillin G. • Pneumococcal pneumonia • Syphilis single treatment with penicillin is curative. No resistance has been reported • gonorrhea
ROUTES : • PENCILLIN V , AMOXICILLIN + CLAVULANIC ACID ORAL • DEPOT : PROCAINE PENCILLIN G, BENZATHINE PENCILLIN G • DO NOT CROSS BBB UNLESS INFLAMED • EXCRETION : TUBULAR SECRETION
SE • HYPERSENSITIVITY—the metabolite penicilloic acid serves as a hapten to cause immune reaction. • Maculopapular rash—ampicillin • Angioedema • anaphylaxis
DIARRHEA– disruption of the normal balance of intestinal micro organisms. Pseudo membranous colitis may also occur. • NEPHRITIS ( Mostly Methicillin) • NEUROTOXICITY– care in epileptics • CATION TOXICITY • Platelet dysfunction ( Carbenicillin & Ticarcillin
Resistance • Beta lactamase enzyme hydrolyzes the cyclic bond of the beta lactam ring—results in loss of bactericidal activity. • Decreased penetration of the antibiotic through the outer cell membrane prevents the drug from reaching the target pbp.
Beta- Lactam Antibiotics Commonly used, some resistance, lower cost Also commonly used, less resistance, higher cost $ $ $ $ Expensive $ $ $ $ Resistant/ Severe Infections SE: all have some degree of cross reactivity w/pen allergic pt. 5-15%
1st Generation • Cefazolin • Cephalexin • Cefadroxil • Cephradine • Broad spectrum, mostly oral, commonly used, some resistance, lower cost, • Active against - Proteus, E. coli, K. pneumonia (PEcK)
2nd Generation • Cefamandole • Cefoxitin • Cefaclor • Cefotetan • Cefuroxime • Less resistance, higher cost, oral/IM/IV. • H. influenza, Enterobacter, Neisseria + 1st (HEN PEcK)
3rd Generation • Cefoperazone • Ceftriaxone • Cefixime • Cefotaxime • Ceftazidime • Expensive, for resistant/severe infections, Septic shock, MENINGITIS.
4th Generation • Cefepime • Newer agent • Very broad spectrum activity
Common usage • Cephalexin - Pharyngitis • Cefazolin - Bone penetration • Cefoxitin – Anaerobes ( Bacteroides fragilis) abdominal sepsis and PID • Ceftazidime – most active against P. aeruginosa • Ceftriaxone – good bone penetration, Neisseria
DISTRIBUTION • BBB: ONLY 3rd GENERATION • MENINGITIS : CEFTRIAXONE, CEFOTAXIME • EXCRETION : RENAL SECRETION (Ceftriaxone, Cefoperazone excreted mostly through bile)
Cephalosporins are mostly not effective against • MRSA, • Listeria monocytogenes • Clostridium difficile • Enterococci. • Newer agent classified as 4th generation (Cefepime) has shown some effectiveness
SE • HYPERSENSITIVITY • CEFOPERAZONE, CEFAMANDOLE – CI IN ALCOHOL • BLEEDING
Beta- Lactam Antibiotics Nephrotoxic Nephrotoxic & Ototoxic
CARBAPENEMS Eg; Imipenem/Cilastatin Cilastatin is not a antibiotic , it’s a peptidase inhibitor that protects imipenem from degradation. Broad spectrum, Mostly IV route and excreted by glomerular filtration. SE: Diarrhea, seizures if increased plasma levels.
Carbapenems • Empiric therapy – active against G positive and negative • Eosinophilia , neutropenia
MONOBACTAMS • Eg; Aztreonam Only in this class. Narrow spectrum – enterobacteria. IV & IM routes , excreted through urine. Relatively non toxic, but can cause skin rash, phlebitis.
Vancomycin • Inhibits synthesis of bacterial cell wall phospholipids and Peptidoglycan • Reserved for serious infections with gram +ve • Used mainly for Methicillin resistant Staphylococcus aureus (MRSA) and Methicillin resistant Staphylococcus epidermidis (MRSE) • And also for antibiotic associated Colitis due to Clostridium difficile or Staphylococci
Slow IV route preferred, • Excretion – glomerular filtration • SE: fever, chills , phlebitis at the site of the injection • Shock reported with fast rapid administration along with Flushing due to histamine release. ( RED MAN SYNDROME)
BETA LACTAMASE INHIBITORS • CLAVULANIC ACID • SULBACTAM • TAZOBACTAM • NO ANTI BACTERIAL ACTIVITY