Download

1 / 16
200 likes | 798 Views
PLATELET DISORDERS. Dr. Hasan Fahmawi, MRCP(UK), FRCP( Edin ). Pethechiae less than 3 mm Purpura 3-10 mm Ecchymosis above 10 mm Red spots, they bleeding into the skin, mucous membranes serosal surfaces, they don’t blanch with pressure Erythematous rash blanch with pressure. Platelets.

E N D
PLATELET DISORDERS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
Pethechiae less than 3 mm • Purpura 3-10 mm • Ecchymosis above 10 mm • Red spots, they bleeding into the skin, mucous membranes serosal surfaces, they don’t blanch with pressure • Erythematous rash blanch with pressure.
Platelets • They are formed in the bone marrow from megakaryocytes. Large numbers of platelets then fragment off from each megakaryocyte into the circulation. The formation and maturation of megakaryocytes is stimulated by thrombopoietinproduced in the liver. Platelets circulate for 8-10 days before they are destroyed by the reticuloendothelial system. • Antiplatelet drugs: aspirin – cyclo-oxygenase inhibitor. • Clopidogrel-adenosine diphosphate (ADP) mediated activation inhibitors. • Dipyridamole - phosphodiesterase inhibitor. • Glycoprotein 11B/111A inhibitors - abciximab which prevent fibrinogen binding.
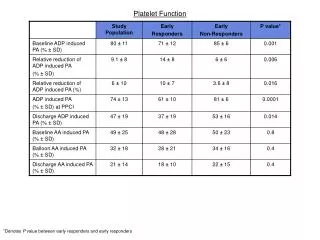
Platelets function assessment • Bleeding time • In vitro by measuring aggregation in response to various agents, such as adrenaline, collagen, thrombin, arachidonic acid, and ADP. • Agglutination in response to ristocetin or by measuring the constituents of the intracellular granules, e.g. ATP, ADP and their ratio to each other ATP/ADP.
Thrombocytopaenia • Decreased or abnormal production(bone marrow failure and hereditary thrombocytopathies) • Increased consumption following release into the circulation(immune mediated, DIC or sequestration. Bleeding doesn’t usually occur until the platelet count falls below 20000, unless their function is also compromised. Purpura and spontaneous bruising are characteristic, but there may also be nasal, oral gastro-intestinaland genitourinary bleeding. Severe thrombocytopaenia below 10000 may result in retinal haemorrhage and potentially fatal intracranial bleeding, but this is rare. Blood film and bone marrow are essential for diagnosis. Treatment depend on the underlying cause
Thrombocytosis • Reactive to another process, presenting features are those of the underlying disease and haemostasis are rarely affected. It is distinguished from myeloproliferative disorders by the presence of uniform small platelets, lack of splenomegaly and the associated disorder. It improves after treatment of the underlying disease.
Platelet function disorders • Bleeding result from platelet disorders, the most common acquired cause is iatrogenic due to antiplatelet drugs. Inherited platelet function disorders are relatively rare. • Glanzmann’s thrombasthenia(11b/111a). • Bernard-Soulier syndrome, 1b • Defective platelet granules, a deficiency of dense(delta)granules giving rise to storage pool disease. • Congenital macrothrombocytopathies are characterized by large platelet, inclusion bodies in the neutrophils, sensorineural deafness and renal abnormalities. • Apart from Glanzmann’s thrombasthaenia, all are benign disorders, with bleeding typically occurring after trauma or surgery, but rarely spontaneously.
Glanzmann’s thrombasthaenia • It is an autosomal recessive condition associate with a variable but usually severe bleeding disorder. Management by local mechanical measures, but antifibrinolytic, such as tranexamic acid, may be useful, and in severe bleeding platelet and blood transfusion might be necessary. Recombinant factor V11 can be used in resistant cases. • Bernard-Soulier syndrome is a hereditary platelet disorder, characterised by thrombocytopaenia, giant platelets, and quantitative platelet defects resulting in bleeding tendency.(easy bruising, epistaxis, menorrhagia, and gastro-intestinal bleeding). • Increase bruising, purpura and petechial rash.
Idiopathic thrombocytopenic purpura • ITP is immune mediated with involvement of autoantibodies(ATP), most often directed against the membrane glycoprotein 11b/111a, which sensetise the platelet, resulting in premature removal from the circulation by the reticuloendothelial cells. It is not a single disorder, some cases occur in isolation while others are associated with underlying immune dysregulation in conditions such as connective tissue diseases, HIV, B-cell malignancies, pregnancy and certain drug therapies. Clinically they are the same.
Clinical features • In adults more common in females and may have more insidious onset, unusual to have history of viral illness. Symptoms or signs of a connective tissue disease may be apparent at presentation or emerge several years later. Patients over 65 years should be considered for bone marrow examination to look for B- cell malignancy, HIV testing is crucial. The peripheral blood film is normal, apart from greatly reduced platelet number, while bone marrow shows marked increase in megakaryocytes. • The presentation depend on the degree of thrombocytopaenia. Spontaneous bleeding occurs only when the platelets are less than 20000. At higher counts , the patient may complain of epistaxis or menorrhagia. • Many cases with counts of more than 50000 are discovered by chance.
Management • If platelets are over 30000 no treatment is required except at times of increased bleeding risk e.g. biopsy or surgery. • In case of bleeding prednisolone 1mg/kg body weight or dexamethasone 40mg daily for 4 days is given, to suppress antibody production or inhibit phagocytosis of sensitised platelets by reticuloendothelial cells. • Immunoglobulin intravenously can raise the platelets and is combined with glucocorticoid therapy if there is severe haemostatic failure. Persistent or potentially life threatening bleeding should be treated with platelet transfusion in addition to other therapies. • In chronic cases relapses should be treated by steroids. If a patient has two relapses or primary refractory disease, second-line therapies are considered. Thrombopoietin receptor agonist(TPO-RA) which produce response in 75% of cases, usually in 10-14 days. Splenectomy induce complete remission in about 70% of cases, and improvement in 20-25% of favourable cases. Low dose steroids and immunosuppressant can be used as well.
Thrombotic Microangiopathies • Acute damage and occlusion of small blood vessels(arterioles and capillaries)in the kidney and other organs. • Microangiopathic haemolytic anaemia, and fragmented RBCs arise as a consequence of passage through the abnormal vessels. • Fragmented RBCs, elevated bilirubin level, raised LDH, reduced haptogloblin (haemolysis). Reticulocytosis, and thrombocytopaenia produced by platelet adherence to the endothelial injury.
Haemolytic Uraemic Syndrome • Thrombotic microangiopathy affecting mainly renal microcirculation. • The most common cause is enterohaemorrhagic Escherichia coli and Shigella dysenteriae. The E. coli 0157;H7 and all which produce verotoxins may be responsible. Dialysis or RRT might be needed for 14 days, and usually is followed by full recovery. • Thrombotic Thrombocytopenic Purpura TTP, it is like HUS characterised by microangiopathic haemolytic anaemia; in contrast ,however, the brain is more commonly affected than kidnies, it is autoimmune disorder caused by antibodies against ADAMTS-13 involved in regulating platelets aggregation and a low; less than 10% serum ADAMTS-13 activity is useful in distinguishing TTP from HUS. as it is treated by plasma exchange.