Download
1 / 65
680 likes | 1.35k Views
Ultrasound-guided fine-needle aspirate and biopsy technique Copyright © 2006 Sound Technologies, Inc. Sound Technologies, Inc. 5817 Dryden Place Carlsbad, CA 92008 1-760-918-9626 www.soundvet.com www.soundveteducation.com Introduction

E N D
Ultrasound-guidedfine-needle aspirate and biopsy technique Copyright © 2006 Sound Technologies, Inc.
Sound Technologies, Inc. 5817 Dryden Place Carlsbad, CA 92008 1-760-918-9626 www.soundvet.com www.soundveteducation.com
Introduction This presentation describes the methods to use as well as other factors to consider when performing an ultrasound-guided fine-needle aspirate (FNA) or core biopsy. The scanning planes used for FNA and core biopsy are the same. The technique varies somewhat, and the differences are demonstrated. Animation is used to demonstrate the aspirate/biopsy techniques. Please note that this animation will not run properly with older versions of PowerPoint or PowerPoint viewer.
Directions In this presentation select the appropriate button on the home page to see the described information. The forward arrow button will take you to the next topic. The back arrow will take you to the prior topic. The ‘home’ button will take you to the home page, and the ‘i’ button will take you to the title page. You may view the animation of each procedure up to three times before having to reset (exit) the presentation. Select a button with under the procedure you would like to view to run the animation. If there are no more buttons seen, you will need to reset the presentation to view that procedure again. To reset the presentation, either press ‘Escape’ on you computer, or select the appropriate button on the home page.
Ultrasound-guided FNA and biopsy technique Method details: Indications Rock/slide the probe Accuracy Keep needle in plane of beam Probe orientation Animal preparation Superficial lesion Screen orientation Materials Deep lesion Reset (exit) program Method References
Indications There are many indications for ultrasound-guided aspirates and biopsies as there are essentially no pathognomonic lesions in ultrasound. Most of the time a cytologic or histopathologic sample is needed to make a definitive diagnosis. Samples for cytology and histopathology may obtained with ultrasound-guided, laparoscopic and surgical procedures.
Indications Icterus/liver enzyme elevation/elevated bile acids Splenomegaly Focal nodules or masses anywhere Renal disease sometimes (i.e. renal dysplasia, renal masses, lymphosarcoma suspects) Prostatomegaly Free abdominal fluid Cysts Lymphadenopathy U/S guided FNA/biopsies generally not done on: Adrenal glands Transitional cell carcinoma suspect masses Chronic renal failure, glomerulonephritis
Accuracy Currently there is a lack of consensus about the accuracy of ultrasound-guided fine needle aspirates and biopsies compared to surgical or post mortem biopsy sample results. Some studies report high accuracy, others, low accuracy. The differential diagnosis and case presentation both should be considered when determining the best method of obtaining a cytology or histopathology sample.
Animal preparation • Coagulation concerns: • A physical examination should be done to assess evidence of a coagulopathy, and if one is suspected, no aspirate or biopsy is recommended. • The pre-biopsy hematocrit should be known. • At least a platelet count is recommended before a fine-needle aspirate is done. • Perform a buccal mucosal bleeding time if i.e. von Willebrand’s disease, or other disorders of primary coagulation are suspected. • A platelet count as well as coagulation profile (PT, aPTT and/or PIVKA) are recommended before a core biopsy is done. • Sedation/brief anesthesia may be indicated. • Prepare a sterile field
Coagulation tests • PT = Prothrombin time • PTT = Partial thromboplastin time • PIVKA = Proteins induced by vitamin K antagonism
Materials • Biopsy guide or not • 22-G 1.5 inch “cysto’ needle or 22-G 3.5 inch spinal needle is often used for fine-needle aspirates. • Attach needle to extension set then syringe for easier handling • 14-G to 18-G core biopsy needles • Bard® automatic biopsy needles • One hand to trigger • Forward ‘throw” varies from 11 to 22 mm • Order from Sound Technologies or other distributors
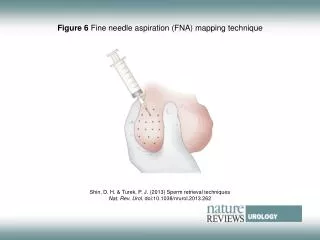
Method • Biopsy guide or freehand • Thickness of beam is 1-2 mm • Must keep needle in plane of beam (biopsy guide would do this for you) • Shortest distance/safest pathway • “Sewing-machine” motion for fine-needle ‘aspirates’ • Stab incision in skin before doing a core biopsy • Sample preparation and evaluation: • Spray aspirates carefully on the slide • Smear gently, dry rapidly • View representative slide before submitting • Place core biopsy samples in cassette, pouch or lens paper • Pick pathologist carefully
Probe orientation Reference marker corresponds to left side of screen (see Screen Orientation slide) Probe Skin Schematic of the resulting ultrasound image Superficial “lesion” to biopsy Deep “lesion” to biopsy
Screen orientation Near field Opposite reference marker Reference marker Far field
Rock and/or slide the probe to line up the lesion to a “reachable” position Superficial lesion can be toward the edge or in the center of the beam Deep lesion needs to be lined up toward the edge of the beam
Keep needle in the same plane as the beam See rotated views
Keep needle in the same plane as the beam: Rotated views of the probe/beam/biopsy plane Needle is placed in the plane of the beam
Angle to use for a superficial lesion: Aim needle more perpendicular to beam FNA: Core biopsy:
Superficial lesion core biopsy Take biopsy
Superficial lesion core biopsy Take biopsy
Superficial lesion core biopsy Take biopsy
Angle to use for a deep lesion: Aim needle more parallel to beam FNA: Core biopsy:
Deep lesion core biopsy