Download

1 / 46
480 likes | 971 Views
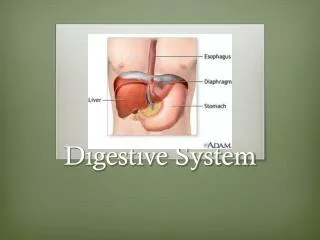
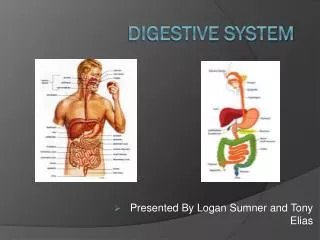
Digestive system. Roles. Digestion Break down food into particles that can be used by the cells Absorb these particles and bring them into the body Eliminate wastes Maintain blood homeostasis Deal with toxins Synthesize blood proteins Regulate blood components.

E N D
Roles • Digestion • Break down food into particles that can be used by the cells • Absorb these particles and bring them into the body • Eliminate wastes • Maintain blood homeostasis • Deal with toxins • Synthesize blood proteins • Regulate blood components
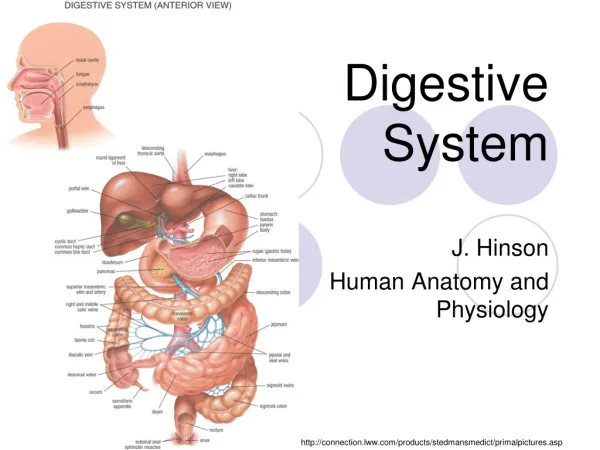
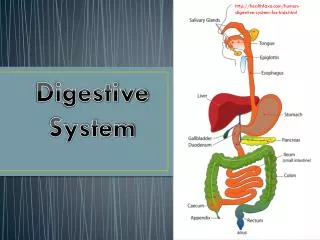
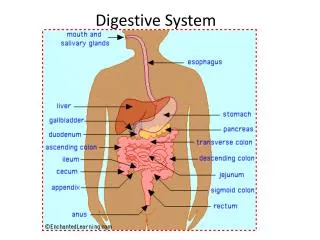
It is the tube that starts at the mouth and ends at the anus The food is processed along this tube This tube is formed by 3 layers. The layer components vary with the location of the track The GI tract
Liver and pancreas These organs secrete enzymes and juices that help digestion Food particles do not enter these organs GI accessory organs
Four basic layers: Mucosa (secretion) – include also a small ring of muscles (muscularis mucosae) with a nervous plexus (submucosal plexus = Meissner’s plexus) Muscular layers (movement) – circular and longitudinal fibers with a plexus, the myenteric plexus (Auerbach plexus) responsible for peristalsis Serosa (protection), connective tissue, for protection is just an extension of the visceral peritoneum GI tract structure
Involuntary Peristalsis Contraction of circular muscle behind the bolus Contraction of longitudinal muscle IN FRONT of the bolus Peristalsis: coordinated contraction of both circular and longitudinal muscle layers of the G.I. musculature as controlled by the enteric nervous system
Involuntary Peristalsis
Enteric Nervous System Submucosal plexus: control secretion Myenteric plexus: control peristalsis
Unique Features • Epithelia of the G.I. tract has a very high turnover/production rate. • Surface epithelia will renew itself every 2-6 days depending on the region of the intestinal tract. • Anti-cancer therapies (targeting rapidly dividing cells) often have the side-effect of targeting the gut as well.
Mouth = oral cavity Cheek, lips, hard & soft palate Lips attached to gums via labial frenulum Palate = roof of oral cavity Hard palate = maxillae & palatine bones Soft palate = muscle-reinforced region dorsal to the hard palate palatine uvula Tongue: move food around & helps for mastication Lingual tonsils can be found at the base of the tongue Mouth = Oral Cavity
Salivary glands • Saliva from 3 paired glands: • Parotid gland (between ear & masseter, largest gland) – innervated by glosspharyngeal (parasympathetic) + T1-T3 of the cervical ganglia of the sympathetic • Submandibular (under middle of mandible) - innervated by facial (VII) nerve (parasympathetic) & T1-T3 of the sympathetic • Sublingual (posterior to submandibular) - innervated by facial (VII) nerve (parasympathetic) & T1-T3 of the sympathetic • Parasympathetic = mucus rich secretion, sympathetic = watery
Muscles involved in mastication: Masseter Temporalis Medial & lateral pterygoid ALL innervated by mandibular branch ofTrigeminal (V) nerve…V3 CN (V) palsy = inability to perform mastication Voluntary Mastication (chewing)
Humans have “heterodont” dentition (various types of teeth) Incisors, canines, premolars & molars Incisors & canines = single root teeth Premolars & molars = multiple roots Mapped using “dental formula” = # incisors, canines, premolars/molars in maxillary portion (assumes everything is equal) = (I 2/2, C 1/1, M 3/3) X 2 Teeth
Humans are also “diphyodont”: 2 sets of teeth during their lifespan Deciduous teeth (milk teeth) begin eruption at 6 months Full set by 2.5 years (full set = 20 teeth) (2/2, 1/1, 2/2) X 2 = 20 teeth Permanent teeth replace deciduous teeth (all the way through late teens) Final formula = (I 2/2, C 1/1, PM2/2, M 3/3) X 2 = 32 teeth Teeth
Crown: above the gum Neck: at the gum (gingiva) level Root: within the bone Outer layer: Enamel the hardest substance in the body, protects tooth. Subject to decay, on the crown only Dentin: softer, throughout the entire tooth Cementum: in the root, outer layer Pulp: made of blood vessels and nerves, present in the pulp cavity Periondontal ligament: attaches the tooth to the bone Teeth - structure
Stratified squamous epithelium (not a “simple” epithelium) Combination of skeletal & smooth muscle (combination of voluntary & involuntary control) Esophagus
Several regions: from lower esophageal sphincter Cardia – fundus – body – antrum Several layers of muscles: longitudinal, oblique and circular Epithelium folded and forming rugae Stomach
Cardia Fundus (storage) Lower esophageal sphincter 3 muscle layers longitudinal, circular, transverse/oblique Body/corpus (acid & pepsin secretion, storage) Pylorus (resistance) Antrum (acid control & mixing)
Chief cells: secrete pepsinogen (inactive precursor to pepsin; protein hydrolase) & prochymosin (precursor to chymosin; coagulates milk) Parietal cells in body/corpus & antrum secrete HCl & intrinsic factor G-cells in the antrum secrete gastrin (endocrine hormone) that triggers both parietal cells & Chief cells Enterochromaffin-like cells (ECL) secrete histamine (works in to magnify gastrin response) Goblet cells secrete mucus Gastric epithelium Epithelium folds and forms pits Along the pits, several types of cells
Small intestine • Three sections: • Duodenum • Jejunum • Ileum • Total length: about 25 feet
Small intestine Small intestine • Surface area: 100-200 m2 ( tennis court) – 25 feet long • greater area for nutrient absorption • cells) • Epithelial surface area is amplified by a number of structures: • Plica muscularis/circularis (2-5X increase in surface area) • Villi (10-30X increase in surface area) • Microvilli of each absorptive enterocyte (200-400X increase in surface area). • Folds of the apical plasma membrane) Plica Villi Microvilli
Duodenum From stomach to jejunum Shortest section, about 20 cm long. Secretions from the pancreas and liver (bile) enter duodenum viaSphincter of Oddilocated in theampulla of Vater (=hepato-pancreatic duct) Region of the intestine where most of food breakdown occurs
Jejunum Important for nutrient absorption Mucosa has many fold, the villi and microvilli increase surface for reabsorption Epithelium is columnar epithelium Within each villus: blood capillaries and 1 lymphatic capillary, the lacteal nutrient reabsorption
Ileum Last section of the small intestine 2-4 m long End at the cecal valve, point of entry into the large intestine Site of absorption of remnants from jejunum, bile salts
Ileocecal Valve • Interface between ileum (terminal small intestine) & large bowel • Acts to limit amount/rate of nutrient entry into the large bowel • Initial “entrance” into large bowel = cecum • Enlarged region of the proximal large bowel • Appendix is located in the cecum • Dense collection of lymph nodes to allow immune system to sample/measure colonic microflora
Large Intestine (colon) Involuntary • Colon (ascending, transverse, descending & sigmoid) serves to absorb electrolytes, and remaining water from the chyme • As water is reabsorbed, the leftover material becomes thicker in consistency stool formation • Colonic epithelia is generally crypt-like; • large capacity to absorb water and electrolytes through surface epithelia • crypt-like architecture also provides enormous secretory capacity
Colonic musculature is unique: • longitudinal muscle layer is “banded” into 2-3tanea coli • circular muscle contracts in “rings”haustraor haustrations • Musculature mixes colonic contents very well
Rectum • For fecal eliminatrion defecation • Presence of 2 sphincters near the anus: • Anal smooth muscle sphincter (involuntary) • Anal striated muscle sphincter (voluntary)
Pelvic diaphragm: support intestines • Levator ani pubococcygeus (anal sphincter), puborectalis, and iliococcygeus. • Coccygeus • Urogenital diaphragm (perineum) • Sphincter urethrea (external sphinter) • Deep transverse perineus
Accessory Gastrointestinal Organs: Liver • Largest internal organ • 4 lobes • Right&left lobesseparated byfalciform ligament • “round ligament/ligamentum teres” attached to falciform ligament = remnant of umbilical vein • Caudate lobeclosest to the IVC • Quadrate lobeadjacent to gall bladder
Liver • Receives blood from the portal vein, from the intestines • Blood is too rich in nutrient and need to be dealt by the liver • Storage of nutrient • Synthesisis of various compact • Detoxification • Blood in homeostatic equilibrium then return to the circulation via the central vein hepatic vein inf. vena cava • Hepatic artery brings oxygen to the liver
Liver: hepatic lobule • The histological/functional units of the liver • Composed of rays of cells with sinusoidal capillaries • Cells = hepatocytes (liver cells) • Interspersed with “Kupffer cells” = resident macrophages • The hepatocytes draw nutrients from the portal vein and store/modify them • They detoxify toxins • They synthesize bile which is collected by the bile ducts
Liver and bile ducts The small bile ducts fuse and form the left and right hepatic ducts The hepatic ducts fuse to become the common hepatic duct The bile, passing into the cystic duct, will be store in the gallbladder When needed (after a meal, the gallbladder will contract and empty the bile into the common bile duct The common bile duct passes around the duodenum, enters the pancreas and fuses with the pancreatic duct to form the hepatopancreatic duct (ampul of vater) The short duct empties into the duodenum through a sphincter, the sphincter of Oddi
Gall Bladder • Stores & concentrates bile • Lined by smooth muscle to aid in contraction during bile mobilization • Can be afflicted by the formation of stones
ERCP Diagnostic Tests: ERCP (Endoscopic Retrograde CholangioPancreatography) To remove gallbladder stones ERCP are done to remove gallbladder stones
Pancreas • Mixed gland (endocrine & exocrine) • Islets of Langerhans= endocrine portion • Pancreatic acini= exocrine portion • Head is peritoneal • Body & tail are secondary retroperitoneal(similar to duodenum) • VERY rich in blood supply • Pancreatic artery & pancreaduodenal branch of the SMA • Exocrine secretions = proteases, carbohydrases, lipases, bicarbonate
Peritoneum Two layer membrane surrounding most organs in the abdomen Outer layer= parietal peritoneum, located against the abdominal wall Inner layer: visceral peritoneum, surrounding the intestines The space between the 2 layers is the peritoneal space has a thin layer of fluid which prevents bowel friction Some abdominal organs are external to the peritoneum (kidneys)
Mesentery Formed by a double layer of visceral peritoneum Binds bowel loop These layers contain blod and lymphatic capillaries as well as nerves going to the intestinal wall The greater omemtum: Large fold over the abdomen The lesser omentum: fold between stomach lesser curvature and liver
Colostomy Sometimes, fecal matter needs to be diverted into a bag because of diseased bowels ileostomy – colostomy
Chronic inflammation of the intestine, most commonly the ileum and cecum areas No known cause Crohn’s disease
Congenital defect where the nerve plexuses within the intestinal wall are missing no peristalsis fecal matter is blocked and accumulates the colon enlarges Hirschsprung disease