Download
1 / 49
670 likes | 1.41k Views
Anatomy of Tonsil and Acute Tonsillitis. Dr. Mubeena. Anatomy of tonsil. Palatine (Faucial tonsil). 2 Lymphoid tissue Location. Palatine tonsil. Medial surface- non keratinising stratified squamous epithelium Crypts – Crypta magna Lateral surface – fibrous capsule

E N D
Anatomy of Tonsil and Acute Tonsillitis Dr. Mubeena
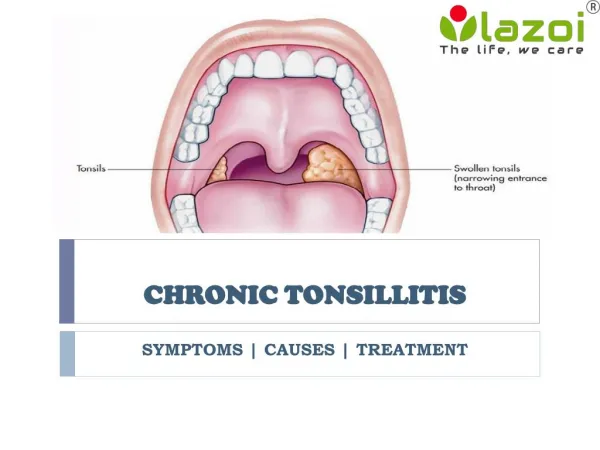
Palatine (Faucial tonsil) • 2 • Lymphoid tissue • Location
Palatine tonsil • Medial surface- non keratinising stratified squamous epithelium • Crypts – Crypta magna • Lateral surface – fibrous capsule • Loose areolar tissue
Palatine tonsil • Upper pole – semilunar fold – supratonsillar fossa • Lower pole – attached to tongue • Tonsillolingual sulcus
Relations of tonsillar bed 1. Tonsillar capsule 2. Peritonsillar space with paratonsillar vein 3. Pharyngo-basilar fascia, Superior constrictor 4. Bucco-pharyngeal fascia 5. Styloid process, muscles, glossopharyngeal nv. 6. Facial artery 7. Medial pterygoid, submandibular salivary gland 8. Mandible
Anatomy of tonsil • Venous drainage:Para tonsillar vein -> common facial vein pharyngeal venous plexus • Lymphatic drainage:jugulo-digastric • Nerve supply:Glossopharyngeal nerve & Lesser palatine nerve
Adenoid Tonsil 1. Ciliated columnar 1. Non-keratinizing epithelium squamous epithelium 2. No capsule 2. Partly encapsulated 3. Has furrows 3. Has crypts 4. Peak growth: 6 yr 4. Peak growth: 8 yr 5. Growth stops: 12 yr 5. Growth stops: 15 yr 6. Disappears: 20 yr 6. Partial regression:18 yr
FUNCTIONS OF TONSILS • 1. LOCAL IMMUNITY • Epithelium • M cells, antigen processing cells antigen brought in contact with subepithelial lymphoid follicles B cell stimulation Plasma cells antibodies
2. Surveillance mechanism • Identifies intruder • Prepares the entire body for defense mechanism
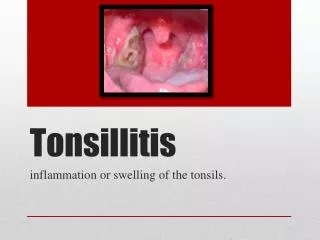
Types of acute tonsillitis 1. Superficial / catarrhal: part of generalized pharyngitis 2. Follicular:crypts filled with pus, visible as yellow-white dots 3. Membranous: multiple follicles join to form a yellow-white membrane 4. Parenchymatous:infection of lymphoid parenchyma tonsil enlargement
Aetiology • Children • Haemolytic streptococcus • Others – Staphylococci, pneumococci, H influenzae
Symptoms • Sore throat • Dysphagia • Fever • Earache • Constitutional symptoms
Signs of tonsillitis 1. Congested tonsil & tonsillar pillars 2. Enlarged tonsil (except chronic fibrotic type) • Follicles over surface of tonsil • White patch/membrane over tonsil 4. Jugulo-digastric lymph node enlarged. Tender jugulo-digastric node seen in acute tonsillitis.
Tonsillar enlargement Grade 1 = tonsil within tonsillar fossa Grade 2= tonsil come outside tonsillar fossa Grade 3 = Significant tonsillar hypertrophy but not touching in midline Grade 4= Kissing tonsils
Complications of acute tonsillitis Local 1. Recurrent tonsillitis 2. Intra-tonsillar abscess 3. Peri-tonsillar abscess (Quinsy) 4. Parapharyngeal abscess 5. Retropharyngeal abscess
Complications of acute tonsillitis Systemic Focal 1. Rheumatic fever 1. Otitis media 2. Endocarditis (SABE) 2. Cervical abscess 3. Glomerulonephritis due to lymph node 4. Urticaria, erythema enlargement 5. Septicemia
Treatment of tonsillitis • Bed rest + plenty of fluids • Systemic antibiotic: Cefadroxil, Cefuroxime • Antihistamine – Decongestant tablet • Analgesics • Antiseptic gargle • Treatment of focus of infection
Membrane over the tonsil tonsil Membranous tonsillitis Faucial diphtheria Infectious mononucleosis Candidiasis (throat swab Candida albicans) Vincent's angina (fusiform bacilli, spirochaete)
Membrane over the tonsil • Aphthous ulcer (red margin, yellow centre) Agranulocytosis (peripheral blood smear) • Leukemia (peripheral blood smear) Neoplasm (excision biopsy) Traumatic ulcer (history of trauma)
Vicent’s angina • Insidious onset • Membrane on one side • Fusiform bacilli, spirochaetes
Infectious Mononucleosis • Young adults • Posterior triangle lymph nodes and splenomegaly • >50 % lymphocytes – 10% atypical • Paul Bunnet test
Faucial diphtheria • Corynebacterium diphtheriae • Droplet infection • Incubation period – 2- 6 days
More in children • Greyish white membrane in oropharynx – bleeds on removal • Jugulodigasric node enlargement – bull neck appearance • Toxaemic
Complications • Due to exotoxins • Myocarditis, arrhythmias, acute circulatory failure • Paralysis of soft palate, diaphragm, ocular muscles • Larynx – airway obstruction
Treatment of faucial diphtheria • Isolation + bed rest • I.V. benzyl penicillin 600 mg q6h 3. Diphtheritic anti - toxininfusion in saline • 20,000 – 40,000 U: 48 hrs duration, tonsillar • 40,000 – 80,000 U: nasopharynx / larynx • 80,000 – 120,000 U: 48 hrs, neck edema 4. Emergency tracheostomy required for stridor
Keratosis pharyngis • Benign self – limiting condition • Etiology: smoking, alcohol, vitamin A deficit • O/E:yellowish, horn-like outgrowths from mucosa of tonsil. Cannot be wiped off. • H.P.E.:Absence of inflammation; hyper-trophy & hyperkeratinization of epithelium.
Keratosis pharyngis Treatment:Reassurance. Tonsillectomy in severe cases.
Diagnosis of membrane over tonsil • History • Physical examination • Total and differential count • Blood smear • Throat swab • Bone marrow aspiration • Paul Bunnet test, biopsy of the lesion
Unilateral tonsillar enlargement Tonsillar causes: 1. Tonsillar malignancy 2. Peri-tonsillar abscess 3. Intra-tonsillar abscess 4. Tonsillolith 5. Tonsillar cyst 6. Tonsillar artery aneurysm 7. Vincent's angina
Unilateral tonsillar enlargement Extra-tonsillar causes: Parapharyngeal abscess Parapharyngeal tumours Tumours of deep parotid lobe Internal carotid art. aneurysm Cervical lymphadenopathy