Download
1 / 44
450 likes | 566 Views
Tonsillitis, Tonsillectomy and Adenoidectomy. Steven T. Wright, M.D. Ronald Deskin, M.D. November 5, 2003. Adenotonsillectomy. Most commonly performed procedure in the history of surgery $500 million annually in healthcare expenditures. History. Almost exclusively by Otolaryngologists

E N D
Tonsillitis, Tonsillectomy and Adenoidectomy Steven T. Wright, M.D. Ronald Deskin, M.D. November 5, 2003
Adenotonsillectomy • Most commonly performed procedure in the history of surgery • $500 million annually in healthcare expenditures
History • Almost exclusively by Otolaryngologists • Celsus in 50 A.D. • Caque of Rheims • Phillip Syng developed the tonsillotome
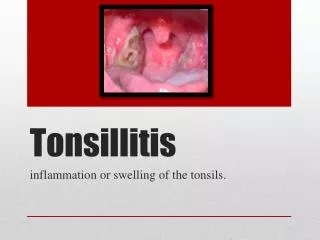
Clinical Evaluation • Acute Tonsillitis • Chronic Tonsillitis • Obstructive Tonsillar Hyperplasia
Clinical Evaluation • Odynophagia, fever, tender cervical lymphadenopathy. • Supporting documents, 2 or more • Fever> 38.5 • Tonsillar Exudate • Tender cervical LAD >2cm • Positive throat culture
Clinical evaluation • Viral • Lower grade fever • Lower WBC, Lymphocytic shift • Less tonsillar exudate • Bacterial • Higher WBC, Granulocytic shift • More exudative
Recurrent Acute Tonsillitis • Seven episodes in a single year • Five or more episodes in 2 years • Three or more episodes in 3 years
Chronic Tonsillitis • No true consensus on the definition. • Symptoms greater than 4 weeks
Differential Diagnosis • Infectious Mononucleosis • EBV • Scarlet Fever • Corynebacterium diptheriae • Malignancy
Complications of Tonsillitis • Cervical Adenitis • Neck Abscess • Peritonsillar abscess • Intratonsillar abscess • Lemierre’s syndrome
Post Streptococcal Glomerulonephritis • Joint Pain and oliguric renal failure 10 days after the pharyngitis. • Treatment aimed at eliminating the infection and supportive therapy for renal failure. • Excellent prognosis in children.
Adenoid Hyperplasia • Triad • Hyponasality • Snoring • Open mouth breathing • Purulent rhinorrhea, post nasal drip, chronic cough, and headache
Obstructive Airway Symptoms • Snoring • Apneic episodes with gasping or choking • Daytime hypersomnolence • Nocturnal enuresis • Behavioral disturbances • Heart failure and Failure to thrive
Tonsil Size • Grade % • 1 <25 • 2 25-50 • 3 51-75 • 4 >75
Obstructive Sleep Apnea • Polysomnography is the gold standard of diagnosis. • Imperative in Adults • In children, a convincing history is adequate • OSA: RDI > 5, SpO2<90% • UARS: RDI <5, SpO2 >90% • Primary Snoring: RDI <1, SpO2>90%
Medical Therapy • TCHP recommends confirming bacterial pharyngitis before beginning antibiotics. • Rapid Strep Test • Throat Culture
Medical Therapy • First Line • Penicillin/Cephalosporin for 10 days • Injectable forms for noncompliance • BLPO, co pathogens • Macrolides • Penicillin allergy • Erythromycin/Clarithromycin 10 days • Azithromycin (12mg/kg/day) 5 days
Medical Therapy • Patients with recurrent otitis media history have higher bacterial concentrations with BLPO. • Initial treatment with anti-BLP antibiotic. • Adenotonsillar size may respond to a one month course of antibiotic therapy. • Adenoid hyperplasia may respond to a 6-8 week course of intranasal steroid.
Surgical Indications • Adenoidectomy • Absolute • Airway obstruction w/ cor pulmonale • Failure to thrive • Relative • Chronic Nasal Obstruction • Recurrent/ Chronic Adenoiditis • Recurrent/ Chronic Sinusitis • Recurrent acute otitis media/ Recurrent COME
Surgical Indications • Absolute • Obstructive airway with cor pulmonale • Severe dysphagia • Failure to thrive • Relative • Recurrent acute tonsillitis • Chronic tonsillitis • Obstructive Sleep Apnea • Peritonsillar Abscess • Halitosis • Suspected Neoplasia/ Tonsillar hyperplasia
Preoperative evaluation • Most common lab test is a CBC • Coagulation studies when the history or physical examination suggests a bleeding disorder. • Lateral Neck/Adenoid films
Von Willebrand’s Disease • Autosomal dominant bleeding disorder • Increased bleeding time and prolonged aPTT. • Perioperative management • IV Desmopressin (0.3ugm/kg) • Serum Sodium
Idiopathic Thrombocytopenic Purpura • Most common thrombocytopenia of childhood. • 90% resolution by 9-12 months • Splenectomy • IVIG preoperatively
Innovative Surgical Techniques • Cold Dissection • Electrosurgery • Intracapsular partial tonsillectomy • Harmonic Scalpel • Radiofrequency tonsillar ablation and coblation.
Electrosurgery • Most popular technique for tonsillectomy • Equivalent or superior to the other methods of tonsillectomy.
Intracapsular Partial Tonsillectomy • 45 degree Microdebrider (1500rpm). • Advantages • As effective as standard tonsillectomy in relieving obstruction. • Less pain, quicker return to normal diet • Disadvantages: • Tonsillar regrowth • Greater intraoperative blood loss
Harmonic Scalpel • Advantages: • Better visibility • Smaller risk of stray energy shocks • Improved post operative pain • Disadvantages: • Must use alternate device for adenoidectomy • Similar intraoperative blood loss.
Radiofrequency tonsillar coblation • Coblation is superior to ablation. • Early elimination of pain and reduced pain medicine usage. • Early resumption of normal diet. • Currently inadequate for adenoidectomy
Adjuvant Therapies Perioperative local anesthetic 0.25% bupivicaine w/ 1:100,000 Epinephrine Advantages: ease of dissection, postoperative pain Disadvantages: Airway obstruction, cardiac dysrrhythmias, seizures
Adjuvant Therapies • Perioperative antibiotics • Fewer episodes of fever, offensive odor, improved oral intake, less pain, fewer days to return to normal activity • Cardiac abnormality
Adjuvant Therapies • Perioperative Steroids • Dexamethasone (0.15-1.0mg/kg) • Two times less likely to have an episode of postoperative emesis, and more likely to advance to eating a soft diet. • Reducing postoperative pulmonary distress, subglottic edema, pain reduction.
Adjuvant Therapies • Pain control • Tylenol and Tylenol w/ codeine are the most commonly used. • Similar pain control, less oral intake with codeine versus Tylenol alone. • NSAIDS still controversial.
Complications • Mortality rate is 1 in 16000-35000. • Anesthetic complications • Eustachian tube injury • VPI • Nasopharyngeal stenosis • Pulmonary Edema • Atlantoaxial subluxation
23 hour observation • Age younger than 3. • Obstructive sleep apnea/craniofacial syndromes involving the airway. • Systemic disorders • Poor socioeconomic situation • Peritonsillar abscess • Emesis or Hemorrhage
Post Operative Hemorrhage • The best treatment is prevention. • Early vs. Delayed hemorrhage. • Overnight observation and venous access • Surgical intervention. • Carotid angiography if any suspicion of carotid artery injury.
Case Study • 8yo male referred to the Pediatric clinic for evaluation and treatment of recurrent tonsillitis.
History • Only 2 episodes of documented pharyngitis in the past 12 months, strep negative, only missed 5 days of school total last year. • Loud snoring, frequent pauses up to 5 seconds terminated with gasps of breath.
Physical Examination • Normal facies, open mouth breathing, tonsils 3+, no cleft deformities. • Remainder of exam is normal.
Case Study • Undergoes uneventful tonsillectomy and adenoidectomy with 23 hour observation. • On follow up visit 2 weeks postoperatively, his mom complains that he doesn’t like some of his favorite foods. He says they taste “yucky”. • Decreased perception of taste with no smell abnormalities.
Diagnosis • Dysgeusia • Unknown mechanism- thought to be due to prolonged pressure on the tongue by the mouth retractor. • Treatment is reassurance.
Bibliography Allen GC, et al. “Adenotonsillectomy in Children with von Willebrand Disease.” Archives of Otolaryngology 1999, May; 125(5) pp547-551. Bailey BJ: Head and Neck Surgery- Otolaryngology, 3rd ed. Philadelphia, Lippincott-Raven, 2001, pp 979- 1006. Brook I, et al. “Microbiology of Healthy and Diseased Adenoids.” Laryngoscope 2000, June; 110(6): pp994-999. Darrow D, Siemens C. “Indications for Tonsillectomy and Adenoidectomy.” Laryngoscope 2002, August; 112(8 part 2): pp6-10. Derkay C, Maddern B. “Innovative Techniques for Adenotonsillar Surgery in Children: Introduction and Commentary.” Laryngoscope 2002, August; 112(8 part 2): p2. Friedman M, et al. “Radiofrequency Tonsil Reduction: Safety, Morbidity, and Efficacy.” Laryngoscope 2003, May; 113(5): pp882-887. Goldstein N. “Child Behavior and Quality of Life Before and After Tonsillectomy and Adenoidectomy.” Archives of Otolaryngology 2002, July; 128(7): pp770-775. Harley E. “Asymmetric Tonsil Size in Children.” Archives of Otolaryngology 2002, July; 128(7): pp767-769. Johnson L, et al. “Complications of Adenotonsillectomy.” Laryngoscope 2002, August; 112: pp35-36. Kay D, et al. “Perioperative Adenotonsillectomy Management in Children: Current practices.” Laryngoscope 2003, April: 113(4): pp 592-597. Koempel J. “On the Origin of Tonsillectomy and the Dissection Method.” Laryngoscope 2002, September; 112(9): pp1583-1586. Koltai P, et al. “Intracapsular Partial Tonsillectomy for Tonsillar Hypertrophy in Children.” Laryngoscope 2002, August; 112 (8 part 2): pp 17-19. Leinbach R, et al. “Hot versus Cold Tonsillectomy: A systematic review of the literature.” Otolaryngology-Head and Neck Surgery 2003, October; 129 (4): pp360-364. Maddern B. “Electrosurgery for tonsillectomy.” Laryngoscope 2002, August; 112(8 part 2): pp11-13. Mui S, et al. “Efficacy of Tonsillectomy for Recurrent Throat Infection in Adults.” Laryngoscope 1998, September; 108(9): pp1325-1328. Plant R. “Radiofrequency Treatment of Tonsillar Hypertrophy.” Laryngoscope 2002, August; 112(8 part 2): pp20-22. Steward D, et al. “Do Steroids Reduce Morbidity of Tonsillectomy? A Meta-analysis of Randomized Trials.” Laryngoscope 2001, October; 111(10): pp1712-1718. Stewart R, et al. “Dexamethasone reduces pain after tonsillectomy in adults.” Clinical Otolaryngology and Allied Sciences 2002, October; 27(5): pp321-326. Thomsen J, Gower V. “Adjuvant Therapies in Children Undergoing Adenotonsillectomy.” Laryngoscope 2002, August; 112(8 part 2): pp32-34. Warltier et al. “Effects of Non-Steroidal, Anti-inflammatory Drugs on Bleeding Risk after Tonsillectomy, Meta-analysis of Randomized Controlled Trails.” Anesthesiology 2003, June; 98(6): pp1497-1502. Wiatrak B, Willging J. “Harmonic Scalpel for Tonsillectomy.” Laryngoscope 2002, August; 112(8 part 2): pp14-16. Younis R, Lazar R. “History and Current Practice of Tonsillectomy.” Laryngoscope 2002, August; 112 (8 part 2): pp3-5.