Download
1 / 42
430 likes | 717 Views
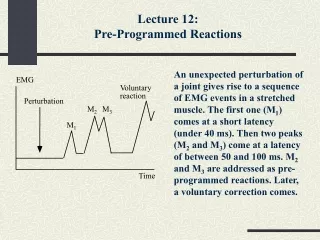
EMG BLIND SPOTS. Know what your EMG might miss!. Introduction. Speakers Tony Chiodo , MD Timothy Dillingham, MD W. David Arnold, MD Shawn Jorgensen, MD. Introduction. Blind spots. Introduction. “ Electrodiagnostic impression : Normal study…”.

E N D
EMG BLIND SPOTS Know what your EMG might miss!
Introduction • Speakers • Tony Chiodo, MD • Timothy Dillingham, MD • W. David Arnold, MD • Shawn Jorgensen, MD
Introduction Blind spots
Introduction “Electrodiagnostic impression: Normal study…”
Generalized peripheral neuropathies “Electrodiagnostic impression: No generalized peripheral neuropathy…”
Generalized peripheral neuropathies • Patient #1 • 29 year old female with one week of numbness, prickly sensation and pain in the feet, progressing to the calves, later in the hands, lips, mouth. • Four days ago began having difficulty going up stairs, getting out of chairs, getting her legs in her pants, getting her arms overhead • Balancing is worsening • No oculobulbar, bowel or bladder symptoms • 2 weeks prior saw PCP, diagnosed with a URI, given a tetanus and influenza vaccine
Generalized peripheral neuropathies • Patient #1 • Physical examination • CN – normal • Motor • 4/5 elbow extension, DIP flexion, ankle dorsiflexion, toe extension, 5-/5 hip flexion • Functionally could not get out of chair without using her arms • Sensory • Pinprick, vibration normal • Romberg positive • MSR • 1+ brachioradialis, others areflexic
Generalized peripheral neuropathies • Patient #1 • Electrodiagnostics • Motor – normal except • Left median to APB: decreased amplitude prox + distally • Right fibular: 25% amplitude loss proximal to distal, decreased CV • Left tibial: prolonged DML, decreased CV • Sensory – normal except • Right sural, bilateral medial dorsal cutaneous prolonged PL • Late responses • F-waves – decreased amplitude ulnar bilaterally, o/w normal • H-reflex – absent bilaterally • NEE • Left upper, lower, paraspinals normal
Generalized peripheral neuropathies • Patient #1 • “Electrodiagnostic Impression: Abnormal study. Mild generalized sensorimotor neuropathy.”
Generalized peripheral neuropathies • Guillain-Barre Syndrome • Acute, autoimmune neuropathy • Clinically presents with acutely progressive sensory dysfunction and weakness, usually in an ascending pattern, progressing for less that four weeks • Exam should demonstrate sensory loss (particularly large fiber), weakness of both proximal and distal muscles, and hyporeflexia
Generalized peripheral neuropathies • Guillain-Barre Syndrome • EMG findings in GBS • Sensorimotor • Non length-dependent • Acquired demyelination • Abnormal temporal dispersion • Conduction block
Generalized peripheral neuropathies • Guillain-Barre Syndrome • EMG findings in early GBS • Demyelination (Albers 1985) • Week 1 - 50% meet full demyelinating criteria • Week 5 – 87% meet criteria • Late Responses – week 1 (Gordon 2001) • 97% abnormal H reflexes (88% day 4) • 87% abnormal F waves
Generalized peripheral neuropathies • Guillain-Barre Syndrome • Non length-dependence • Abnormal upper limb/normal lower limb • “Sural sparing” • 50% of patients by week 1 (Gordon 2001)
Generalized peripheral neuropathies • EMG BLIND SPOTS!! • Guillain-Barre syndrome • Early normal/minimally abnormal EDX • Look for late responses • Normal sural • Look for abnormal upper limb
Generalized peripheral neuropathies • Patient #1 – revised impression • “Electrodiagnostic Impression: Abnormal study. Mild generalized peripheral neuropathy; cannot exclude early AIDP • Clinical Impression: Monitor closely for worsening neurological symptoms and repeat NCS in one week if symptoms don’t improve or worsen. Consider consultation with a neuromuscular specialist.”
Generalized peripheral neuropathies • Patient #2 • 67 year old patient with slowly progressive ambulatory decline • Thinks it has been going on for 3 years • Feels weakness is in his legs and has some in arms as well • When asked, notes numbness in feet and hands • No oculobulbar or sphincter complaints • PMH: DM2, mild CHF
Generalized peripheral neuropathies • Patient #2 • Physical examination • Cranial nerves - normal • Motor – normal excepts • 3+/5 right, 4/5 left arm abduction • 4/5 finger abduction • 2/5 hip flexion • 4/5 knee extension • 4/5 right, 3-/5 left ankle dorsiflexion • MSR • Trace in uppers, 0 in lowers • Sensation • Absent vibration at ankles • Pinprick normal
Generalized peripheral neuropathies • Patient #2 • Electrodiagnostics • Motor NCS • Diffusely diminished conduction velocities • Dramatic temporal dispersion across the forearm on right ulnar motor • Lower limb studies unobtainable • Sensory NCS • Lowers unobtainable • Ulnar sensory low amplitude • Needle EMG • Abnormal spontaneous activity, large amplitude MUAP in distal LE muscles
Generalized peripheral neuropathies • Patient #2 • “Electrodiagnostic Impression: Abnormal study. Generalized sensorimotor neuropathy with axonal and demyelinating features.”
Generalized peripheral neuropathies • CIDP • Chronic inflammatory demyelinating polyradiculoneuropathy • MS of the PNS (Amato 2009) • Autoimmune • demyelinating • often relapsing/remitting course, other progressive • More common than you think! • Of those with cryptogenic neuropathy referred for intensive referral center investigation, about 1/5 have CIDP (and are treatable) (Dyck 1981)
Generalized peripheral neuropathies • CIDP • Clinical features • Progresses for 8 weeks or more • Weakness classically proximal and distal, symmetrical • Hyporeflexia • Sensory complaints • Lab features • EDX – diffuse sensorimotor acquired demyelination (similar to AIDP) • CSF – cytoalbuminic dissociation
Generalized peripheral neuropathies • CIDP • Atypical forms • Not all meet even basic clinical features • Asymmetrical or pure sensory in 50% cases (Breiner 2014)
Generalized peripheral neuropathies • CIDP • Criteria (AAN) • Clinical • Motor and or sensory loss in >1 limb • Hyporeflexic • Over 2 months • Electrodiagnostic • 3 out of 4 • CB/TD in >=1 nerve • CV decreased in >=2 nerves • DL prolonged in >=2 nerves • FW prolonged in >=2 nerves
Generalized peripheral neuropathies • CIDP • Criteria • At least 15! • No consensus • Sensitivities range from 11-91% (Breiner 2014) • False negatives – treatable patients missed • Specificity range from 63-100% (Breiner 2014) • False positives – non-treatable patients exposed to unnecessary risks, MAJOR costs • Of those with treatable disease (by expert consensus), about 1/3 never met ANY criteria (Bromberg 1991)
Generalized peripheral neuropathies • Patient #2 • Diagnostics • CSF analysis • Protein 97, otherwise normal • Treatment • Moderate improvement with IVIg • Strength improved to >=4/5 proximal muscles • Reflexes 2+ uppers, patella • Able to ambulate with walker and minimal assistance
Generalized peripheral neuropathies • BLIND SPOTS!! • CIDP • Not meeting criteria • Consider those with basic clinical features • Asymmetrical, no proximal and distal weakness • Consider asymmetrical, pure sensory forms
Generalized peripheral neuropathies • Patient #2 – revised impression • “Electrodiagnostic Impression: Abnormal study. Generalized peripheral neuropathy with features of acquired demyelination; suspicious for but not meeting research criteria for chronic inflammatory demyelinating polyneuropathy (CIDP)” • “Clinical Impression: This patient may have a non-classic form of CIDP. Consultation with a neuromuscular specialist and lumbar puncture could be considered.”
Generalized peripheral neuropathies • Patient #3 • 47 year old with 2 months of cramping, numbness and tingling on the anterolateral ankle and dorsal foot • Has had numbness in the right hand for years • Balance is fine • No orthostatic hypotension, constipation, nausea • Strength is normal • Blurry vision, otherwise no oculobulbar complaints or trouble controlling her bowel or bladder
Generalized peripheral neuropathies • Patient #3 • Physical examination • Cranial nerves – normal • Motor exam – normal • Sensory exam • Decreased pinprick sensation in the distal foot, otherwise normal • Normal vibration, light touch, temperature sensation • Reflexes - normal • Coordination - normal
Generalized peripheral neuropathies • Patient #3 • Electrodiagnostics • CMAP – normal median, ulnar, fibular • SNAP – normal sural, medial dorsal cutaneous, median, ulnar, radial • NEE – normal UE/LE
Generalized peripheral neuropathies Pictures of EDX
Generalized peripheral neuropathies • Patient #3 • “Electrodiagnostic impression: Normal study. No generalized peripheral neuropathy or lumbosacral radiculopathy.”
Generalized peripheral neuropathies • Subtle neuropathies • EDX techniques to increase sensitivity • Medial plantar • Mild diabetics – 50% with prolonged sural latency, 70% prolonged/absent medial plantar (Reeves 1984)
Generalized peripheral neuropathies • Small fiber neuropathy • Sensory fibers for pain, temperature, autonomic fibers • Clinical presentation with pain, burning • Usually no numbness, tingling, weakness • Physical examination • Loss of pinprick and temperature sensation with normal light touch, proprioception and vibration • Normal strength • Normal MSR
Generalized peripheral neuropathies • Small fiber neuropathy • Studies • Electrodiagnostics – normal!!! • Skin biopsy • Measurement of intraepidermal nerve fiber density • Decreased in 77% of patients at the distal calf with clinical suspicion of small fiber neuropathy (Holland 1998) • Autonomic testing • Different tests, yields
Generalized peripheral neuropathies • EMG BLIND SPOTS!! • Subtle neuropathies • Consider tests with increased sensitivity (medial plantar) • Small fiber neuropathy • Remember standard EDX only tests large fibers
Generalized peripheral neuropathies • Patient #3 – revised impression • “Electrodiagnostic Impression: Normal study. No generalized peripheral neuropathy affecting large fibers. • Clinical Impression: A neuropathy primarily affecting small fibers cannot be excluded with standard electrodiagnostic studies. Specialized testing (skin biopsy, autonomic testing) could be considered to further assess this possibility.”
Generalized peripheral neuropathies • EMG BLIND SPOTS!! – summary • GBS • Be aware of low yield in early testing – use H-reflex • Be aware of non length-dependent findings (sural sparing) • CIDP • Be aware of low sensitivity of research criteria • Be aware of relatively high frequency of atypical presentations • Possible subtle neuropathies • Consider testing with increased sensitivity (i.e. medial plantar) • Remember small fiber neuropathies have negative EDX!
Generalized peripheral neuropathies Thank you!!
References Asbury AK, Cornblath DR. Assessment of current diagnostic criteria for Guillain-Barre syndrome. Ann Neurol 1990;27(suppl):S21-S24. Albers JW, Donofrio PD, McGonagle TK. Sequential electrodiagnostic abnormalities in acute inflammatory demyelinatingpolyradiculoneuropathy. Muscle Nerve 1985;8:528-539. Gordon PH, Wilbourne AJ. Early electrodiagnostic findings in Guillain-Barre syndrome. Arch Neurol 2001;58:913-917. Amato AA, Russell JA. Neuromuscular disorders. New York: McGraw Hill Medical; 2008. Dyck PJ, Oviatt KF, Lambert EH. Intensive evaluation of referred unclassified neuropathies yields improved diagnosis. Ann Neurol 1981; 10: 222-226. AAN – change to EFNS Breiner A, Brannigan TH. Comparison of sensitivity and specificity among 15 criteria for chronic inflammatory demyelinatingpolyneuropathy. Muscle Nerve 2014;50:40-46. Bromberg M. Comparison of electrodiagnostic criteria for primary demyelination in chronic polyneuropathy. Muscle Nerve 1991;14:968-976. Reeves ML, Seigler DE, Ayyar DR, et al. Medial plantar sensory response. Sensitive indicator of peripheral nerve dysfunction in patients with diabetes mellitus. Am J Med 1984;76(5):842-846. Holland NR, Crawford TO, Hauer P, Cornblath DR, Griffin JW, McArthur JC. Small-fiber sensory neuropathies: clinical course and neuropathyology of idiopathic causes. Ann Neurol 1988;55(1):47-59.