Download
1 / 20
200 likes | 318 Views
Implementing High Impact Prevention in South Carolina. Wayne A. Duffus, M.D.; PhD Medical Director, STD/HIV Division South Carolina (SC) Department of Health and Environmental Control. The Problem.

E N D
Implementing High Impact Prevention in South Carolina Wayne A. Duffus, M.D.; PhD Medical Director, STD/HIV Division South Carolina (SC) Department of Health and Environmental Control
Percent Priority Populations Reached with ILI/GLI*2010-2011 compared to the Percent of New HIV/AIDS Cases 2009-2010 by Priority Population, (HIV Prevention and Expanded Testing (non-clinical) contractors) % Priority Populations ILI: Individual Level Interventions; GLI: Group Level Interventions
Percent of Priority Populations Reached with CTRS in 2010-2011 Compared to the Percent of New HIV/AIDS Cases 2009-2010(HIV Prevention and Expanded Testing (non-clinical) Contractors) % Priority Populations Counseling, Testing and Referral (CTR) Services
Many SC HIV-Infected Persons Access Health Care But Are Not Tested • All reported cases of HIV, 2001 – 2005 confidentially matched with registry of health care visits during 1997-2005 • 4,315 reported HIV cases • 3,157 (73%) made 20,271 health-care visits prior to their first positive HIV test; median 4 visits • Diagnosis codes at 15,648 (77%) of prior visits would not have prompted an HIV test • 1,784 (42%) developed AIDS within 1 year of HIV test MMWR 55:47, December 1, 2006
Overall Proportions Linked to HIV Care in SC After New Diagnosis * ‘Not in Care’ is no visit within 12 months after diagnosis
SC Priority Populations*(at high risk for infecting others or getting infected with HIV) • HIV Positive Persons (CDC mandated) • African American Men who have Sex with Men (AAMSM) • African American Women who have Sex with Men (AAWSM) • African American Men who have Sex with Women (AAMSW) • White Men who have Sex with Men (WMSM) • Injection Drug Users (IDU) • Hispanics *Source: SC HIV Prevention Plan: Chapter 3
SC Priority Interventions Categories* Defined prior to High Impact Prevention: • Counseling, Testing and Referral (CTR) Services • Partner Services (PS) • Comprehensive Risk Counseling and Services (CRCS) • Individual Level Interventions (ILI) • Group Level Interventions (GLI) • Community Level Interventions (CLI) • Health Communication/Public Information (HC/PI) • Outreach • Capacity Building (CB) • Social Networking Strategies (SNS) *Source: 2012-2014 SC HIV Prevention Plan: Chapter 3
SC Priority Interventions* Emphasizing High-Impact Prevention (CY2012) • HIV Testing (targeted and routine) • Prevention with Positives • Condom Distribution • Behavioral Interventions for High-Risk Negatives • Policy and other structural interventions
SC Preventions Funds were Awarded in Alignment with the National HIV/AIDS Strategy Focus HIV prevention efforts in communities and local areas where HIV is most heavily concentrated to achieve the greatest impact in decreasing the risks of acquiring HIV. Increase targeted HIV testing in non-healthcare settings to identify undiagnosed HIV infection, with a program minimum of at least a 1.0% rate of newly identified HIV positive tests annually. Increase access to care and improve health outcomes for people living with HIV by linking them to continuous and coordinated quality care and much needed medical, prevention and social services. Expand targeted efforts to prevent HIV infection using a combination of effective, evidence-based approaches, including delivery of integrated and coordinated behavioral and structural HIV prevention interventions. Reduce HIV-related disparities and promote health equity.
SC Eligibility Requirements to Receive HIV Prevention Funding Within the past three years, have a minimum of at least a three-year documented history of providing HIV testing services to one or more of South Carolina’s priority populations. Documentation of a minimum of .05% HIV testing positivity rate in a 12-month, calendar year service period and maintaining a 1% positivity rate once funded. Have current documentation of a CLIA waiver for conducting HIV testing, staff with current HIV testing credentials, and documentation of quality assurance protocol and service procedures for HIV testing. Have at least a one-year documented history of providing group-level, CDC-identified, evidence-based interventions (EBIs) to persons living with HIV/AIDS (PLWHA), if proposing to deliver Healthy Relationships and/or WiLLOW.
SC Eligibility Requirements to Receive HIV Prevention Funding Have at least a two-year documented history of delivering Many Men, Many Voices (3MV) to African American men who have sex with men (AAMSM), if proposing to deliver 3MV. Provide documentation of collaborating with the local health department(s), specifically in regards to conducting HIV Counseling, Testing and Referral Services (CTRS), STD screenings, TB prevention activities, Hepatitis B virus (HBV) and Hepatitis C virus (HCV) CTRS, and Hepatitis A/B vaccine services or service referrals.
Regions in South Carolina Where HIV Prevention Services are Offered Community-based (Targeted) Prevention Services Red = Top 11 counties for numbers of new HIV infections and the number of persons living with HIV. *All red areas will have targeted services funded. Yellow = Other areas being funded for targeted services. All counties (red, yellow, green) have STD/HIV prevention services (testing, screening and partner services (disease intervention) through local health department.
SC Prevention Shifts in Funding to Community Based Organization (CBOs) In addition, in CY2012: Funding allocations for targeted testing by CBOs account for 58% of overall funding awards Funding allocations for prevention with positives by CBOs account for 22% of overall funding awards Funding allocations targeted to AAMSM account for 67% of the funding for behavioral interventions to HRN
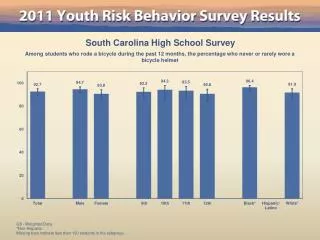
HIV Testing Information by Race and Ethnicity from Health Department Testing Sites, 2011 Total number of tests = 45,250 **Includes Asian/Pacific Islander and American Indian/Alaskan Native The overall positivity rate from all tests done at health department sites in 2011 was 1.0%
HIV Testing Information by Risk Group from Health Department Testing Sites, 2011 The overall positivity rate from all tests done at DHEC sites in 2011 was 1.0 percent
Comparison of HIV-infected Individuals Diagnosed from 2004-2006 and 2008-2010 • Demographics • 70.7% Male • 70.1% Black • 41.2% MSM • 72.2% resided in urban areas at diagnosis • Persons from 2008-2010 were more likely to be linked to care within 3 months than those from 2004-2006 (p<0.0001) • Persons diagnosed in 2008-2010 were less likely to be in care after 12-months than within 3-months (aOR 0.28, 95%CI=0.22-0.35)
Comparison of HIV-infected Individuals Diagnosed from 2004-2006 and 2008-2010 • Persons diagnosed in 2008-2010 were more likely to have • CD4 counts >500 than <200 • CD4 counts between 350-500 than <200 • A year after diagnosis, individuals from 2008-2010 were more likely to maintain • CD4 counts >500 than <200 • CD4 counts between 350-500 than <200 • Have an undetectable viral load • Those diagnosed in 2008-2010 were more likely to have AIDS at the time of diagnosis (aOR 1.30, 95%CI=1.11-1.51); however no significance one year after diagnosis in AIDS disease stage