Download
1 / 83
1.67k likes | 3.84k Views
SPLENECTOMY & COMPLICATIONS. Roshin Reeba Joseph. SPLENECTOMY & COMPLICATIONS. Indications Preoperative preparations Open splenectomy Laparoscopic splenectomy Hand assisted laparoscopic splenectomy Postoperative complications. Indications for splenectomy. Trauma Oncological

E N D
SPLENECTOMY & COMPLICATIONS Roshin Reeba Joseph
SPLENECTOMY & COMPLICATIONS Indications Preoperative preparations Open splenectomy Laparoscopic splenectomy Hand assisted laparoscopic splenectomy Postoperative complications
Indications for splenectomy • Trauma • Oncological • Haematological • Portal hypertension • Cysts , tumours and abscesses
Splenic trauma • Penetrating trauma • Blunt trauma • Intra operative • spontaneous
Splenic rupture • Acute – immediate intraperitoneal bleed. • Delayed – after days or weeks. • Occult – traumatic pseudocyst . • Splenosis
Trauma • Signs & symptoms depend on bleeding. • Tachycardia, hypotension & kher’ s sign. • Investigations : • Diagnostic peritoneal lavage : >100,000 Rbc’s • CT • FAST • Rx : • spontaneous rupture of diseased organ do splenectomy. • Iatrogenic lacerations : splenic repair.
Scale to assess splenic injury • Class I : 1. Nonexpanding subcapsular haematoma < 10% surface area. 2. nonbleeding capsular laceration with parenchymal involvement < 1cm deep.
Class II : 1. Nonexpanding subcapsular haematoma 10-50 % surface area. 2. nonexpanding intraparenchymal haematoma < 2cm diameter. 3. bleeding capsular tear or parenchymal laceration 1-3 cm deep without trabecular vessel involvement.
Class III : • expanding subcapsular or intraparenchymal hematoma. • Bleeding subcapsular haematoma or a haematoma > 50 % area. • Intraparenchymal haematoma > 2 cm diameter. • Parenchymal laceration > 3 cm deep or involving trabecular vessels.
Class IV : 1. Ruptured intraparenchymal haematoma with active bleeding. • Laceration involving segmental or hilar vessels producing major ( > 25% ) splenic devascularization.
• Class V : • Completely shattered or avulsed spleen. • Hilar laceration which devascularises entire spleen.
Rx : class I, II , III – conservative Rx. class IV – splenic conservation class V - splenectomy.
Haematological disorders • Thrombocytopenia • Haemolytic anaemias • Hypersplenism • Lymphomas
Thrombocytopenia • Immune thrombocytopenic purpura • If there is inadequate response to steroids • Relapse after an initial remission • If the disease has lasted more than a year. • Thrombotic thrombocytopenic purpura • If there is inadequate response to plasma exchange. • Helps prevent relapse. • Hemolytic uraemic syndrome.
Haemolytic anaemias • Hereditary spherocytosis • Splenectomy indicated in all patients. • Not performed in routine cases before six years. • Indications for an earlier splenectomy • aplastic crisis • growth failure • severe anaemia.
Hereditary elliptocytosis • Idiopathic autoimmune haemolytic anaemia. • Sickle disease • Thalassemias • Pyruvate kinase deficiency.
C f Hereditary spherocytosis Hereditary elliptocytosis
schistocytes Sickle cell disease
Hypersplenism • Primary hypersplenism • Secondary hypersplenism • Portal hypertension • Leukaemias • Inflammatory, infiltrative conditions • Felty’s syndrome • Gaucher’s disease. • Myelofibrosis
LYMPHOMAS • Ann arbor staging : A – asymptomatic B - fever ,night sweats & weight loss E – extralymphatic S - spleen.
I – localised to a single lymph node or nodal group. • II – more than 1 nodal group on the same side of the diaphragm. • III – more than 1 nodal group on both sides of the diaphragm. • IV- spread to organs other than the lymph node and the spleen
Splenectomy in lymphomas • Hodgkin’s lymphoma : • Stage IA , IIA – radiation. staging laparotomy is indicated in these patients where the results will affect the medical management. staging laparotomy involves a thorough abdominal exploration, splenectomy, liver biopsy, bone marrow biopsy, multiple lymph node sampling.
Stage IVA & all B – chemotherapy. MOPP regime or ADVB. • Stage IIIA – either treatment. 2. Non Hodgkins lymphoma.
Cysts • Parasitic • Non parasitic
Parasitic cysts • 2/3 of cysts in the spleen • Majority hydatid cysts – echinococcus. • Treatment : 1. splenectomy or 2. resection of the roof of the cyst with splenic salvage. • High risk : mebendazole 10 mg/kg/day p.o. for 2 weeks & cyst aspiration followed by inj. with hypertonic saline & reaspiration.
Non parasitic cysts • True cysts • Pseudocysts
Pseudocysts • 2/3 of the nonparasitic cysts • No epithelial lining • Traumatic hematoma formation with absorption. • C/F : left upper quadrant pain radiating to the shoulder. • If < 5 cm : USG follow up, resolves. • If > 5 cm : splenorrhaphy or partial excision with marsupialization. • Splenectomy if salvage not possible.
True cysts • Epithelial lining • Mostly congenital. • Epidermoid & dermoid cysts • symptomatic : if < ½ size of the spleen : splenic salvage. if > ½ size : splenectomy
Tumours • Primary rare. • Mets : breast, lung, melanoma. • Vascular: most common primary. Majority benign haemangiomas or lymphangiomas , no Rx needed. But if splenomegaly present do splenectomy. 2. Hamartomas
hemangioma hamartoma
Tumours ( contd.) • Splenic lymphomas • Localised to spleen and surrounding retroperitoneal lymph nodes. • No peripheral involvement. • Adjuvant chemo or radiotherapy.
Splenic abscesses • 2/3 due to seeding from distant septicemic focus : endocarditis , UTI.. • Post trauma, hemoglobinopathies, contiguous spread. • C/F : fever, abdominal discomfort, splenomegaly. • Investigations: X-ray, USG , CT. CT : low homogenous density with edges that do not intensify on i/v contrast.
Rx : 1. antibiotics after cultures. 2. unilocular: percutaneous drainage & antibiotics. 3. splenectomy with post op antibiotics definitive Mx. 4. fungal : antifungals alone.
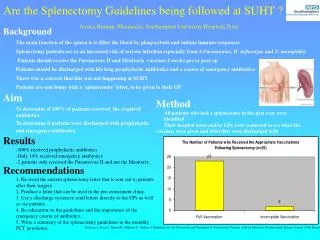
Pre operative preparations • Vaccinations : • pneumococcal vaccine given 2 wks pre op to > 2 yrs. Repeat 6 yrs after splenectomy. > 2 yrs : pneumovax 6 wks – 2 yrs : prevnar. • Meningococcal vaccine to > 2 yrs. • Hib vaacine if not taken in infancy. • Influenza vaccine. • In emergency splenectomy it should be administered in the early post op period.
Contd…. • Platelets tranfused after splenic artery is clamped. • Steroids contd. if needed. • In myeloproliferative disorders, better to medicate with low dose heparin( 5000 IU s/c BD.) & antiplatelet drugs like aspirin on day before surgery.Contd 5 days post op.
Orogastric tube put into stomach after endotracheal intubation. • IgG transfusion. • FFP • Splenic artery embolisation in high risk cases : eg. massive splenomegaly due to myelofibrosis.
Types of splenectomy • Elective splenectomy • Emergency splenectomy
Types of splenectomy • Open splenectomy • Laparoscopic splenectomy • Hand assisted laparoscopic splenectomy
ABSOLUTE INDICATIONS • Unsalvagable & life threatening splenic trauma • ITP with intracranial hemorrhage • Primary malignancy or secondaries • Heriditary spherocytosis • Sinistral portal hypertension • Hairy cell leukemia
OPERATIVE TECHNIQUES • INCISION 1.Upper midline 2.Left oblique subcostal 3.Thoracoabdominal
PROCEDURE - elective • Transecting the ligamentous attachments - splenophrenic lig. Superiorly,inferiorly spleno colic & spleno renal lig.followed by blunt dissection • 2 or 3 short gastric vessels from spleen to greater curvature of stomach is ligated in contuinuity & divided • Spleen delivered into wound by blunt dissection posteriorly
Contd……. • Not to divide post attachments to far medially to avoid entering splenic V • Avoid axial rotation of spleen to avoid disruption of splenic vein & artery • Dissection carried out at the hilum as close to the spleen as possible to avoid injury to pancreas • Individual ligation of splenic A & its branches and splenic V & its branches is preferable
Contd……. • Splenic A ligation is double ligation and suture ligature • Splenic V double ligated and divided • Large spleen put vascular clamps and lumen closed with continuous vascular sutures • Hemostasis with special attention to three areas – inferior surface of diaphragm, greater curvature of stomach and region of short gastric vessels , region of hilus
Contd……. • In hematological disorders exploration for accessory spleen is needed • Usually in the following sites - hilus , gastrosplenic lig. ,Gastrocolic lig. , greater omentum , mesentry , presacral space