Download
1 / 39
390 likes | 1.01k Views
Suspected Drug-Induced SLE, APLS and ANCA Vasculitis. Rheumatology winter clinical symposium 2019 Nina narasimhalu , md. CASE PRESENTATION. 33-year-old male presents with bilateral lower extremity edema, progressive myalgias , generalized weakness, periorbital swelling and rash for 2 weeks

E N D
Suspected Drug-Induced SLE, APLS and ANCA Vasculitis Rheumatology winter clinical symposium 2019 Nina narasimhalu, md
CASE PRESENTATION • 33-year-old male presents with bilateral lower extremity edema, progressive myalgias, generalized weakness, periorbital swelling and rash for 2 weeks • Patient also reports history of progressive shortness of breath, which was evaluated 10 days prior to presentation at an outside hospital (work-up was incomplete since he left AMA), productive cough, sore throat and loss of appetite • Denies photosensitivity, pleurisy, hematuria, foaming/frothing of urine • Positive exposure to sick contacts (niece had upper respiratory tract symptoms)
HISTORY • No past medical history • No prior surgeries • Allergy to Bactrim • Social history notable for tobacco (1/2 pack per day for 10 years), frequent intravenous heroin and methamphetamine use, skin popping • Last IVDU was 1 day prior to admission
LABS in ED • WBC 7.2, Hgb 9.7, platelets 97 • Absolute lymphocytes 1.5, absolute neutrophils 5.1 • Na 126, K 4.2, Cl 99, CO2 21, BUN 55, Cr 1.2, glucose 107, calcium 7.5 • AlkP 53, AST 147, ALT 43, Tbili 0.7, total protein 5.8, albumin 2.3 • UA with 100 protein, moderate Hgb, 7 WBC, 4 RBC • CRP 5.1 mg/dL, ESR 59 • INR 1.18 • Lactic acid 1.0 • Troponin 0.03
PHYSICAL EXAM • T 98.1F, HR 122, RR 32, BP 111/65, 93% • General: Restless and uncomfortable. • HEENT: Periorbital edema bilaterally with overlying erythema. • Chest/CV: Diminished breath sounds. Tachycardic, regular rhythm. • Abd: Normoactive bowel sounds. NT, ND. • Ext: 2+ edema of BLE extending above knees. • MSK: No active synovitis. • Skin: Dermatitis with flaking of skin of distal bilateral lower extremities. Erythematous maculopapular rash on anterior chest. Flaking of skin on scalp. Violaceous palpable and non-palpable macules on feet extending to toes with retiform pattern. Right lateral thigh with healing eschar vs non-draining wound.
IMAGING • CXR: Moderate cardiomegaly. No focal pulmonary consolidation. No large pleural effusion or gross PNX. • US BLE: No DVTs. • US Abd: Mild HSM. Moderate pericardial effusion. Small bilateral pleural effusions. • TTE: Echo evidence of impending cardiac tamponade. Moderate pericardial effusion. Normal LVEF. RVSP 20.8mmHg. • CT Chest: Mild to moderate pleural effusion on L with collapse of L lower lobe. Small to moderate pleural effusion on R. Prominent mediastinal LNs.
Moderate pericardial effusion with small bilateral pleural effusions.
CLINICAL COURSE • Pericardiocentesis with removal of 650mL of serosanguinous fluid and placement of pericardial drain additional 1L drained • At this time, differential had included infectious etiology with post-nephrotic syndrome • Due to intermittent fevers, Infectious Disease service was consulted infectious work-up remained negative NO antibiotics • Skin biopsy of purpuric lesion on R foot concerning for vaso-occlusive process vs vasculitis • Nephrology was consulted as UPC 0.9 24-hour urine with 1.8g/24 • At this point, there was a high index of suspicion for SLE
CLINICAL COURSE CONTINUED • Increased work of breathing requiring BiPAP and HiFloNC • Developed pAF and was started on amiodarone • Drop in Hgb 7.3 6.6 with elevated haptoglobin and normal Tbili • Re-consulted ID due to fevers repeat endocarditis and infectious work-up largely negative • Ended up starting antibiotics when sputum culture grew Staph aureus and UCx grew E. faecalis • At this point, labs were notable for a positive ANA, low complements, +Coomb’s, cytopenias AND with patient’s serositis, renal insufficiency with proteinuria, patient met diagnostic criteria for SLE • After much discussion with family, decision made to begin Solumedrol 125mg IV daily
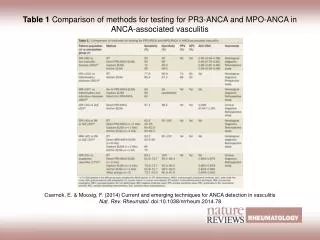
UPDATED RHEUMATOLOGY LABS • ANA 1:320 homogenous • dsDNA 1:2560 • Histone 7.8 (+) • NEG Smith, RNP, SSA, SSB, Jo-1 • C3 18.7, C4 7 • p-ANCA 1:320 with MPO 63 and PR3 37 • Cardiolipin IgG 69, IgM 56, LAC weakly positive, Beta-2 IgG 119, IgM <5 • Ferritin 2128
CLINICAL COURSE • Worsening pulmonary edema and atrial fibrillation with RVR intubated for 2 days then extubated • Underwent thoracentesis with removal of 1L fluid • Now admitted to cocaine use too • Underwent renal biopsy to further elucidate etiology SLE vs ANCA • Discharged home after biopsy on prednisone 60mg daily • Total hospitalization: 17 days
PATHOLOGY of SKIN • FINAL DIAGNOSIS AFTER MICROSCOPY: SKIN, RIGHT LATERAL FOOT, PUNCH BIOPSY: OCCLUSIVE VASCULOPATHY WITH VASCULAR NECROSIS (SEE COMMENT) PAS SPECIAL STAIN IS NEGATIVE FOR FUNGUS. Comment: Thrombotic vasculitis can be seen in patients taking cocaine contaminated with levamisole and in autoimmune diseases (lupus, antiphospholipid syndrome, anti-cardiolipin antibodies).
RENAL BIOPSY PATHOLOGY • UCLA FINAL DIAGNOSIS KIDNEY, NATIVE (NEEDLE CORE BIOPSY): - Focal proliferative glomerulonephritis with moderate activity including focal crescents (see COMMENT) - Acute tubular injury and tubulointerstitial inflammation, favor secondary to glomerulonephritis - Mild global glomerulosclerosis, no interstitial fibrosis/tubular atrophy, and moderate arterial sclerosis - No evidence for thrombotic micrangiopathy
RENAL BIOPSY IMMUNOFLUORESCENCE Courtesy of UCLA
RENAL BIOPSY PATHOLOGY Courtesy of UCLA
POST-HOSPITALIZATION • Returned 2 days after discharge for volume overload hospitalized for 3 days for diuresis • Went to 1 post-hospitalization follow-up appointment, but no-showed 2 of his rheumatology follow-up appointments • Came back 2 months after initial hospitalization complaining of SOB and BLE swelling, had gone back to using IV drugs, including methamphetamine and heroin, had been off of prednisone x 1 month echocardiogram showed constrictive pericarditis creatinine elevated, dsDNA > 5120, low complements started on Solumedrol acutely then transitioned to prednisone upon discharge, also started on Plaquenil and CellCept 500mg PO BID
POST-HOSPITALIZATION COURSE • Returned 1 month after that discharge complaining of SOB, had started using intravenous heroin again found to have multiple pulmonary emboli and bilateral thigh abscesses s/p I&Ds • Patient was restarted on a lower dose of prednisone to help support him through infection due to concern for adrenal insufficiency, CellCept was held, discharged home with antibiotics, Plaquenil and prednisone • Did not come to post-hospitalization Rheumatology appointment • Returned 5 months later and was admitted for 1 week had Pseudomonas and S. pneumoniae PNA and was receiving antibiotics but patient left AMA • Found to have new onset cardiomyopathy with EF 34% during this admission
MOST RECENT HOSPITALIZATION • Patient had left against medical advice, but continued to feel unwell so he came back to the ED a few days later … • Started on empiric antibiotics and heart failure therapy • Decompensated and briefly intubated for a day, creatinine steadily rising • Became hypoxic a few days later and was re-intubated had a bronchoscopy, which confirmed diffuse alveolar hemorrhage • Started on Solumedrol 125mg q6h • Transfusion Medicine consulted for possible plasma exchange • Successfully extubated 3 days later and admitted to ongoing drug use • Had been clean for 3 months, but fell back into old habits 2-3 days before admission
Diffuse bilateral ground glass opacities, smooth interlobular septal thickening, lower lobe predominant consolidative opacities.
CLINICAL COURSE • Discharged to acute rehabilitation unit with a prednisone taper • Close outpatient follow-up appointment scheduled (within a few days) • If patient shows up, we can discuss immunosuppressive therapy options
THE QUESTIONS THAT CAME UP … • Is patient’s underlying autoimmune disease (SLE, APLS and AAV) related to his drug use? • Isn’t drug-induced disease typically non-organ threatening? • Are his labs consistent with what we might see with drug-induced disease? • Could it be levamisole?
LEVAMISOLE • Levamisole is an antihelminthic agent used in veterinary medicine • Removed from the US market in 2000 due to adverse effects • Popular adulterant of cocaine • Per DEA report, approximately 70% of cocaine contained levamisole in 2009 • Has also been found with other illicit substances, such as heroin Brunt, et al. Casale, et al. Lee, et al.
LEVAMISOLE and COCAINE • Looks similar to cocaine! • Can be used as a cutting or bulking agent can increase weight of sample make drug appear purer • Unclear physiologic effect when both are combined • Theories include: • Prolong cocaine-induced euphoria via nicotinic acetylcholinergic effects on CNS? • Act as an indirect serotonin agonist? Brunt, et al. Lee, et al.
HISTORY OF LEVAMISOLE • Was used as a DMARD for RA in the 1970s • Was used with 5-FU for colon cancer in the 1990s • Removed from US market in 2000 and Canadian market in 2003 due to reports of agranulocytosis Lee, et al.
MECHANISM OF ACTION • Immunomodulator increase macrophage chemotaxis and T-cell lymphocyte function • Stimulate neutrophil and monocyte chemotaxis increase inflammatory responses • Up-regulate toll-like receptors • Enhance dendritic maturation and function of macrophages • Increased cytokine production (IL-1) • Metabolite aminorex exhibits amphetamine-like effects on dopamine and norepinephrine transporters • Acts as a central mediator in mice changes metabolism of norepinephrine, serotonin and dopamine Brunt, et al. Lee, et al.
LEVAMISOLE-TOXICITY • Can be characterized by the following: • Cutaneous manifestations: • Retiform purpura • Hemorrhagic bullae • Necrosis • Commonly involves face, bilateral helixes, cheeks, nose • Case reports mention other areas of involvement throughout body • Vasculitis (with immune complex deposition) vs pseudovasculitis Lee, et al.
OTHER SYMPTOMS of LEVAMISOLE-TOXICITY • Arthralgias • Large joints • Generalized fatigue and malaise • Constitutional symptoms • Renal failure • Pulmonary hemorrhage • Pulmonary HTN • Leukoencephalopathy Brunt, et al. Lee, et al.
LAB ABNORMALITIES • Agranulocytosis* • Neutropenia, leukopenia • +ANA (in speckled pattern, most often) • +dsDNA, +LAC • Normal complements • +ANCA, +MPO > + PR3 (but can have both) • Anti-human elastase antibody sensitive and specific for levamisole-induced vasculitis Brunt, et al. Hennings, et al. Lee, et al.
PATHOLOGY OF SPECIMENS • Skin biopsies: • LCV • TMA • Panniculitis • Necrosis • Renal biopsies: • Pauci-immune focal necrotizing crescentic GN Brunt, et al. Hennings, et al. Lee, et al.
PHARMACOKINETICS of LEVAMISOLE • Cocaine remains in urine for 48-72 hours • Hard to necessarily tie cocaine use and levamisole together • Levamisole quickly absorbed with short half-life (5.5-6 hours) • Extensively metabolized in the liver • Highest concentrations of levamisole found in blood and lung tissue • Women affected more than men? Brunt, et al. Lee, et al.
PROGNOSIS OF LEVAMISOLE-ASSOCIATED DISEASE • Generally good, but it depends on patient’s willingness to stop using drugs that contain the offending agent: • Cocaine • Heroin • Sometimes, it is necessary to use immunosuppressive therapy such as high-dose steroids, Cytoxan or MMF • Plasmapheresis has been used too in severe cases • Plaquenil for skin and joint-related disease Rivera, et al. Striebich.
NOTABLY FOR OUR PATIENT • His lupus anticoagulant, anti-cardiolipin IgG/IgM and beta-2 glycoprotein IgG/M are now negative and his pulmonary emboli have resolved • But in light of continued drug use, do we continue with anti-coagulation? Did being clean for 3 months prior to relapse have any effect on his serologies? • Systemic Lupus Erythematosus in 6 Male Cocaine Users at Bellevue Hospital by Rivera et. al discussed an interesting topic: • Can we learn more about disease pathogenesis of SLE in men who abuse cocaine?
TAKE HOME POINTS • Not only is levamisole being used to adulterate cocaine, but it is also found in heroin! • Levamisole has been associated with SLE, APLS and ANCA-vasculitis • Cocaine is not only adulterated with levamisole, but diltiazem too, which is another cause of drug-induced SLE • Heroin can also be adulterated with griseofulvin, which has been associated with drug-induced SLE • Anti-elastase antibody is both sensitive and specific for levamisole-induced vasculitis Broseus, et al. Brunt, et al. Lee, et al.
ACKNOWLEDGMENTS • Patient provided verbal consent to present his case and emphatically agreed that “everyone should be aware of this!” • UCI Department of Rheumatology
REFERENCES • Borchers AT, Keen CL, Gershwin ME. Drug-induced lupus. Ann N Y Acad Sci. 2007 Jun;1108:166-82. • Broséus J, Gentile N, Esseiva P. The cutting of cocaine and heroin: A critical review. Forensic Sci Int. 2016 May;262:73-83. • Brunt TM, van den Berg J, Pennings E, Venhuis B. Adverse effects of levamisole in cocaine users: a review and risk assessment. Arch Toxicol. 2017 Jun;91(6):2303-2313. • Casale EM, Casale JF. Identification of levamisole and lidocaine acetylation reaction impurities found in illicit cocaine exhibits. Microgram J. 2011; 8(1):16-23. • Hennings C, Miller J. Illicit drugs: What dermatologists need to know. J Am AcadDermatol. 2013 Jul;69(1):135-42.
REFERENCES • Lee KC, Ladizinski B, Federman DG. Complications associated with use of levamisole-contaminated cocaine: an emerging public health challenge. Mayo Clin Proc. 2012 Jun;87(6):581-6. • McGrath MM, Isakova T, Rennke HG, Mottola AM, Laliberte KA, Niles JL. Contaminated cocaine and antineutrophil cytoplasmic antibody-associated disease.Clin J Am SocNephrol. 2011 Dec;6(12):2799-805. • Rivera TL, Belmont HM, Weissmann G. Systemic lupus erythematosus in 6 male cocaine users at Bellevue hospital. J Rheumatol. 2009 Dec;36(12):2854-5. • Striebich, C. Chapter 17: Drug Induced Lupus. Rheumatology Secrets. Sterling G. West. Philidelphia: Elsevier/Mosby, 2015. 137-140.