Download
1 / 36
380 likes | 409 Views
Explore the intricate relationship between sleep apnea and cardiovascular disease, delving into how both impact each other and the need for more research. Discover the prevalence of sleep disorders in cardiac patients and their risks. Learn about the association between sleep apnea, hypertension, heart failure, and arrhythmias, emphasizing the importance of screening and treatment. Uncover the consequences of untreated sleep apnea on the cardiovascular system.

E N D
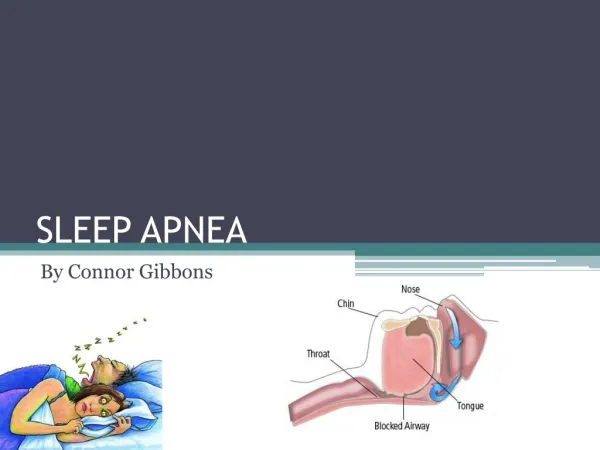
Sleep Apnea in the Cardiac Patient Stephen Jennison
What is the impact of Sleep apnea on cardiovascular disease? • Which came first: sleep apnea or CV disease? • More research is needed per AHA and ACC • Difficult to decide impact due to multiple co- morbidities of obesity, diabetes and metabolic syndrome
SDB Impact on the Cardiovascular System • Both OSA & CSA occur commonly in patients with cardiovascular disease and HF and may contribute to disease progression.
Sympathetic Parasympathetic Constrict Dilate Stop secretion Secrete saliva Spinal cord Parasympathetic Constrict bronchioles Dilate bronchioles Sympathetic ganglion chain Speed up heartbeat Slow down heartbeat Secrete adrenaline Increase secretion Adrenal gland Decrease secretion Stomach Increase motility Decrease motility Empty colon Retain colon contents Empty bladder Delay emptying Bladder Parasympathetic
Arousal & Hyperventilation O2 & CO2 Decreased Compensation Airway Patency Compensation O2 & CO2 Airway Collapse Sympathetic Activation Sympathetic Activation Increased RR Wakefulness Increased mental activity Increased BP HR Increased Sleep Increased release of glucose
OSA OSA Impacts: Sympathetic Nerve Activity, Blood Pressure, Oxygenation etc. Sympathetic Nerve Activity RESP OSA OSA 250 BP 125 0 Somers VK et al. J Clin Invest. 1995;96:1897.
Prevalence of Sleep Disordered Breathing in Cardiovascular Disease • 30% of cardiac disease patients • Schafer et al, Cardiology 1999 • 50% of heart failure patients • Javaheri, Circulation 1998 • 40% pts with systolic HF • 50% pts with diastolic HF • 30% of hypertensive patients • 83% of refractory hypertension • Logan et al, J Hypertension 2001
Association BetweenOSA & Hypertension • 40- 60% of patients with HTN have OSA2 • 85% of patients with Resistant Hypertension on 3 or more meds have OSA • Even mild OSA is a risk factor for hypertension3, 6 • Patients with untreated OSA may be resistant to their anti-hypertensive medications4 • Even small decreases in blood pressure may help to decrease the risk of heart attack and stroke5 ¹Silverberg, et al., Curr Hypertens R 2001 2 Kraicze, et al., AJRCCM 2000 3 Bixler, et al., Arch Intern Med 2000 4 Logan, et al., J Hypertens 2001 5 Heinrich, et al., Circulation 2002 6 Neito, et al., Jama 2000
Hypertension Guidelines • Recommendation by Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC 7): • Sleep Apnea listed identifiable cause of Hypertension • All newly diagnosed patients should be screened for Sleep Apnea • All patients with refractory hypertension should be screened for Sleep Apnea Chobanian, AV et al., J Hypertens 2003; 42: 1206-1252
Association BetweenOSA & Heart Failure • 37% of 450 HF patients had OSA • Also high incidence of Central or Mixed apneas • Risk factors for OSA in HF included • BMI > 35 in males • Age > 60 in females Sin et.al, Am J Respir Crit Care Med 1999; 160: 1101-1106 Work by Sin, et al., 2000
Shaded bar: pts with OSA White bar: pts. without OSA Association BetweenOSA & Arrhythmias • The prevalence of arrhythmias was compared in two samples of participants from the Sleep Heart Health Study • 228 subjects with sleep-disordered breathing (RDI > 30) vs. 338 subjects without sleep-disordered breathing (RDI < 5) • Individuals with severe sleep-disordered breathing have two to fourfold higher odds of complex arrhythmias than those without sleep-disordered breathing even after adjustment for potential confounders. Mehra R, et.al. Am J of Respir Crit Care Med 2006 Vol. 173: 910-916
ACC/AHA HFSA Heart Failure Guidelines • Recommendation by American College of Cardiology, American Heart Association and the Heart Failure Society of America : • Sleep Apnea listed identifiable cause of Heart Failure • It is recommended that all newly diagnosed patients be screened for Sleep Apnea • Patients refractory to treatment for Heart Failure should be screened for Sleep Apnea Hunt, et.al. ACC/AHA 2005 Guidelines: Circulation:2005:112
Cardiovascular mortality and morbidity in OSA • Study of 1651 Men, over 10 years • 264 Normal (control group) • 377 Snorers (AHI<5) • 403 Untreated Mild-Mod OSA (AHI 5 – 30 without EDS) • 235 Untreated Severe OSA (AHI > 30 or AHI> 5 with EDS) • 372 Severe OSA with CPAP Treatment OSA (AHI > 30, CPAP > 4hrs/day) • CPAP compliance objectively measured • Study Fatal and Non-Fatal Cardiac Events Marin, JM et. al Lancet 2005: 365:1046 - 1053
Fatal CV Events over 10 year period Marin, JM et. al Lancet 2005: 365:1046 - 1053
Non-Fatal CV Events per group Marin, JM et. al Lancet 2005: 365:1046 - 1053
Outcomes of Study • Patients with severe OSA that was left untreated had a significant increase in CV events (both fatal or non-fatal events) after 10 years • Risk factor: 2.87 higher than norms • Patients with severe OSA had a significant reduction in CV events when treated with CPAP • Patients who used CPAP > 4 hours per night had a drop in CV risk Marin, JM et. al Lancet 2005: 365:1046 - 1053
Treatment of OSA & Refractory HTN • 16 of 19 refractory HTN patients had underlying OSA • 11 patients participated in CPAP trial • CPAP titrated to approx. 9 cm H20 • Blood pressure and baroreflex sensitivity were studied on and off CPAP • 24-hourblood pressure was evaluated at baseline and after 2 months of CPAP therapy • Logan AG., et al., Eur Respir J 2003; 21: 241-247
Results: • CPAP group: Approximate 10mmHg drop in mean blood pressure • predicts a 37% reduction in risk for CHD • 56% reduction in risk for stroke • No relevant change in blood pressure occurred with sub-therapeutic CPAP
Screening in Hospital • Sleep apnea is found in at least 50% of patients with CHF • Heart Failure nurses should screen for sleep apnea in all CHF patients • Referral to sleep disorder team • Outpatient sleep study per MD order All cardiac patients in outpatient Cardiology clinic should be screened with Epworth Sleepiness tool
Results: Treatment of OSA & Refractory HTN Logan AG., et al., Eur Respir J 2003; 21: 241-247
Hallmark OSA Signs and Symptoms • Excessive daytime sleepiness (EDS) unexplained by other factors with • Loud disruptive snoring or • Nocturnal choking/gasping/snorting or • Nocturnal pauses in breathing
Additional Signs/Symptoms of OSA • Recurrent nocturnal awakenings • Un-refreshing sleep • Daytime fatigue • Impaired concentration/memory loss • Mood/behavioral changes • Morning headaches • Loss of sexual interest
Pearls • If person is on 3 antihypertensive medications and still has high blood pressure, consider a sleep study • When a person has “congestive heart failure” due to fluid buildup and their BNP is less than 120, screen for sleep apnea • Newly diagnosed CHF patients should be screened for sleep apnea early • Atrial fibrillation patients should be screened • All cardiac patients should be screened when no other known cause for cardiac condition
Suggestions for cardiac patients to use CPAP/ BIPAP • Use humidifier on CPAP to prevent dryness • Nasal spray to open air passages • Wear during naps to get used to mask and get a boost of energy for rest of the day • Encourage support from spouse/SO • Give CPAP a friendly name • Use at least 4 hours per night for benefit
Great News • Treatment can give people a new lease on life • More energy • Relieve headaches • Control blood pressure • Sleep all night • Less strain on the heart • Reduces cardiac events • Improve CHF symptoms
Sleep Trivia on Internet sites • 3,150,000 sites for sleep apnea • Oral Appliances that mold to your mouth • Exercises to “cure” sleep apnea $19.99