Download
1 / 31
340 likes | 950 Views
Endometrial Cancer. Adrienne Kassis, M.D. April 20, 2010. Case 1: Nervous Nelly. 67 y/o Caucasian female with hypertension and osteopenia presenting for her annual physical exam Pan-positive ROS INCLUDING:

E N D
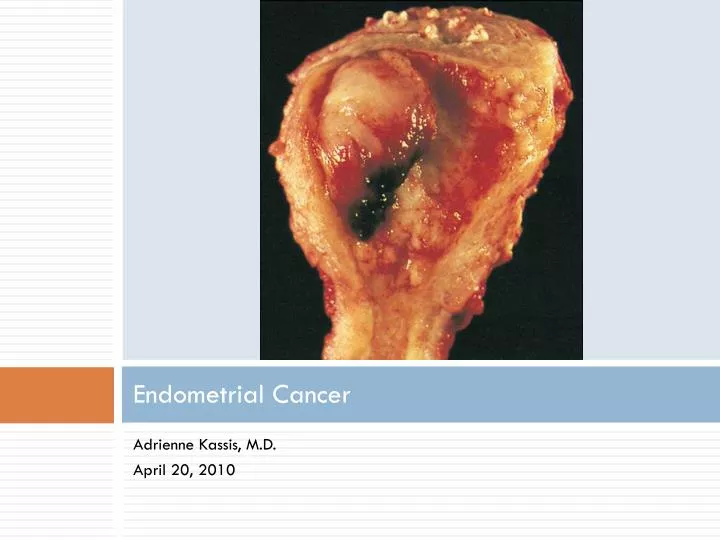
Endometrial Cancer Adrienne Kassis, M.D. April 20, 2010
Case 1: Nervous Nelly • 67 y/o Caucasian female with hypertension and osteopenia presenting for her annual physical exam • Pan-positive ROS INCLUDING: • “Last year I noticed a drop of blood on my underwear but I was too scared to tell you about it” • Would you pursue this? • If so, how would you evaluate her?
Case 2: Unlucky Ursula • 32 y/o F presents for a new patient appointment • PMHx • Anxiety • Hyperthyroidism • Colon cancer dx age 27 s/p partial colectomy • FHx • Paternal GM ovarian cancer and colon cancer • Thoughts?
Case 3: Plump Patty • 36 year old female presents with irregular menses • Inter-cycle spotting • Occasional heavy periods with clots • 5-6 periods per year • BMI = 34 • Jawline acne • Infertility • What are your initial thoughts about this patient? How might you treat her?
Endometrial Carcinoma: Background • Most common gynecologic cancer in the U.S. • 6% of all cancers in women • Incidence is highest in Caucasians • Mortality twice as high in blacks • 2.5% lifetime risk • Cure rates are high • 96% five year survival for localized disease
Epidemiology • 90% of cases in women over 50 • Median age of diagnosis age 62 • Mortality rate • 4 deaths per 100,000 women per year
Histopathology • Type 1 • Low grade • Endometrioid tumor • Association with atypical hyperplasia • Estrogen-related • Clear risk factors • Type 2 • Higher grade • Papillary serous/clear cell tumors • Unrelated to estrogen • Unclear risk factors • Usually occur in older patients
Risk Factors • Long-term estrogen exposure • (in the absence of adequate progestins) • Diabetes and hypertension • Age • Genetics • History of breast cancer • Nulliparity • Early menarche/late menopause
The Role of Estrogens Endogenous Exogenous • Chronic anovulation • Obesity • Estrogen-secreting tumors • Hormonal replacement therapy (unopposed) • Tamoxifen
Protective Factors • OCPs • Coffee • Physical activity • Postmenopausal progestins • Smoking!
Clinical Presentation • Abnormal uterine bleeding • Pre-menopausal • Post-menopausal • Abnormal cervical cytology • Endometrial cells in patients > 40 years old
Who to test? • Post-menopausal women with ANY amount of vaginal bleeding • Pre-menopausal women over the age of 35 with “abnormal uterine bleeding” • This includes: menorrhagia, menometorrhagia, mid-cycle spotting • Pre-menopausal women age 30 or older with Lynch syndrome • (or 5-10 years prior to first Lynch-associated cancer in any family member) • Pre-menopausal women under the age of 35 with prolonged abnormal bleeding despite treatment • Women over the age of 40 with endometrial cells on Pap smear
Lynch Syndrome • HNPCC (hereditary nonpolyposis colorectal cancer) • Autosomal dominant germline mutation in one of four DNA mismatch repair genes • 1/3100 ages 15-74 • Lynch patients have: • 27-71% risk of endometrial cancer • 3-14% risk of ovarian cancer
Workup • Physical Exam (including BMI and pelvic exam) • Labs (CBC, U preg, TSH, pap, STD screen) • Diagnostic tests • Endometrial biopsy • Hysteroscopy with D and C • Transvaginal Ultrasound • Sonohysterography
Workup • Endometrial biopsy • Outpatient procedure using a Pipelle • Sensitivity: 99% post-menopausal; 91% pre-menopausal • Specificity: 87% • PROS: • Simple to perform • Well-tolerated • No anesthesia • High sensitivity, low complication rate, low cost • CONS: • Invasive • Uncomfortable • Less useful for localized cancers
Workup • Transvaginal Ultrasound • Helps to distinguish atrophy from anatomic lesions needing biopsy • Gives a measurement of the endometrial stripe • Less than 4-5 mm: low risk of disease • 20 mm: avg thickness in women with cancer
Workup • Transvaginal Ultrasound • PROS: • Noninvasive • May help the patient avoid biopsy • CONS: • Less useful in premenopausal patients • Lower sensitivity and specificity (67% and 56%)
Workup • Hysteroscopy with D and C • Occasionally requires anesthesia • Associated with a higher rate of complications • Sonohysterography • Saline infusion into the uterus • Helps to identify focal abnormalities in order to do a targeted biopsy • Often used as a second step
Which to choose first? • ACOG: either TVUS or EMB may be used as initial test • IF endometrial stripe is less than 4 mm, EMB is not required.
Diagnosis • Requires direct tissue sampling via biopsy or D&C for confirmation
Treatment • Endometrial hyperplasia • Without atypia • With atypia • Endometrial cancer • TAH/BSO • Peritoneal washings • +/- chemo and radiation
Screening • NOT recommended for: • General population • Women on tamoxifen • Obese women • Caveat: Women with Lynch syndrome • Start age 30-35 OR 5-10 years prior to first Lynch-associate cancer in the family • Annual endometrial sampling +/- TVUS • Prophylactic TAH/BSO in women who have completed childbearing • Consider chemoprevention with OCPs
Take-Home Points • Pre-menopausal women can get endometrial cancer! • Even ONE drop of blood in a post-menopausal woman is a symptom that merits workup • Endometrial cells on a pap are not always a benign finding • Keep Lynch syndrome in the back of your head