Download
1 / 33
330 likes | 719 Views
甲状腺激素和抗甲状腺药 Thyroid hormones and antithyroid drugs. 北京协和医学院基础医学院药理学系 叶菜英. Summary Thyroid hormones Necessary to maintain normal metabolism, growth and development. Hypothyroidism Cause Cretinism if it happens in embryo or neonatal period.

E N D
甲状腺激素和抗甲状腺药Thyroid hormones and antithyroid drugs 北京协和医学院基础医学院药理学系 叶菜英
Summary • Thyroid hormones Necessary to maintain normal metabolism, growth and development. • Hypothyroidism Cause Cretinism if it happens in embryo or neonatal period. Cause myxedema if it happens in adults when the thyroid hormone could be used in replacement therapy. • Hyperthyroidism A syndrom characterized by thyroid oversecretion and metabolic disorder caused by multiple reasons. It can be treated with radioactive iodine (131I) irradation, antithyroid drugs and operation.
Thyroid hormones • Thyroxine, T4 • Triiodothyreninum natricum, T3 Synthesized and secreted by thyroid
抗甲状腺药 分为4类: • 硫脲类 Thiourea • 碘和碘化物 (复方碘溶液, lugol’s solution)) • 放射性碘(131I) • β受体阻断药(心得安等从略)
硫脲类 • 硫氧嘧啶类(thiouracil): • 甲基硫氧嘧啶(methykthiouracil) • 丙基硫氧嘧啶(propylthiouracil) • 咪唑类(imidazoles) • 他巴唑(Tapazole,甲巯咪唑methimazole) • 甲亢平(卡比马唑Carbimazole)
Thyroid hormones • Thyroid hormones are iodic amino acids • Active components Thyroxine, T4 Triiodothyreninum natricum, T3 • Chemical constitution
Physiological disposition of thyroid hormones • Absorbed rapidly when take orally , activity T3>T4,maintaining time T4>T3. T1/2 of T4 and T3 are 6-7 days and 1-2 days, respectively. • Deiodination in mitochondria of liver and kidney, eliminated by kidney affer conjugated with glucuronicacid and sulfuric acid. • T3, T4 can also pass the placenta and enter milk. • Figure: the amount of normal adults’ thyroid hormones produced and metabolized daily.
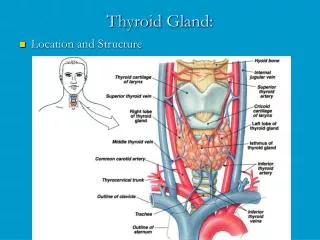
Synthesis, storage and regulation of thyroid hormones • Iodine uptake • Iodine activation and tyrosine iodation • Condensation and storage • Disintegration and release • Regulation
Steps of thyroid hormones synthesis, release and regulation (Ⅰ) • Iodine uptake: I-in blood can be uptaken into cells by iodine pump in the adenocyte membrane . The amino acids can be used to synthesize thyroid globulin in cells. • Iodine activation and tyrosine iodation: I-uptaken into cells can be oxydized to active iodine by peroxydase. Active iodine binds to tyrosine of TG and forms monoiodotyrosine (MIT) and diiodotyrosine (DTT).
Steps of thyroid hormones synthesis, release and regulation (Ⅱ) • Condensation and storage: In the thyroid globulin molecule , two DTTs are condensed to T4 , one DTT and one MIT are condensed to T3,which are all stored in gland alveolus colloid . • Disintegration and release: T3 and T4 are released into blood after hydrolyzed by proteases .At the same time , some of them can be turned back to tyrosine and I- by deiodinase in cells and reused. • Regulation: By the positive and negative feedback regulation of hypothalamus-anterior lobe-thyroid axis. Hypothalamus secrets TRH ,anterior lobe secrets TSH and thyroid synthesize T3 , T4.
Synthesis, storage and release of thyroid hormone Gastrointestinal I- Acinar lumina T3 T3 MIT+DIT MIT Con-den-sation Protease Iodation TG Peroxidase I- Io BloodI- DIT T4 T4 DIT+DIT TG Tyr MIT 一碘酪氨酸 DIT 二碘酪氨酸 TG 甲状腺球蛋白 blood Activation Synthesis Storage Release
Thyroid hormones Mechanism of action • The binding of T3 and R increases the uptake of aa and glucose, resulting in the entrance to cytoplasm of T3. After reacting with CBP, T3 is educed. The free T3 can bind R in the mitochondria and make ADP to ATP. Besides, it can enter the nuclear and bind R there, which can increase the transcription of DNA and the content of mRNA. Then the new proteins can be synthesized and play roles.
Thyroid hormones • Mechanism of action(figure) • It is believed now that the thermogenic action of T3 and T4 is due to the increase of sodium pumps activity on the cell membrane . Na+,K+—ATPase activity ATP utilization ADP concentration mitochondria respiration oxide consumption and heat production
Physiological and pharmacological actions • Keep normal growth and development Promote synthesis of proteins as well as growth and development of skeleton and CNS. T3, T4 deficient secretion: causes cretinism in infants and young children and mucous edema in adults. • Promote metabolism and increase heat production Promote oxidation, increase oxygen consumption, basal metabolic rate and heat production. • Elevate sensitivity of sympathetic - adrenal system Nervousness, trembling, heartbeat speed up, blood pressure increase
Thyroid clinical application Replacement therapy mainly Therapy and diagnosis Application • CretinismTreating the infants and children as soon as possible could cure them to normal . If treating too late, they need to be treated a lifetime. • Mucous edema Increase the dosage of thyroid pallet gradually . Too large dosage may aggravate heart diseases . Patients in coma should be given a fist aid, which is infusion of T3 (40-120μg)intravenoiusly , reinjection 5-15μg every 6h and oral administration when awake. Hypopituitarism patients should be given cortical hormone first and followed by thyroid hormone. • Simple goiter Replacement therapy can inhibit TSH oversecretion and contract the glandular organ, 3-6 months. • T3 inhibition test Differential diagnosis for Patients with iodine high uptake.
Adverse effects Adverse effect Overdose Contraindication Combination old people heart disease diabetes hypertension Coronary heart disease pyknocardia hyperthyreosis bishydroxycoumarin dantina or aspirin thyroid crisis: anxiety, fear, restlessness, high body temperature, increase and irregular heart rate, increase pulse pressure, congestive heart failure with vomit, diarrhea and dehydration which lead to coma and death Angina or heart infarction Increase toxicity of thyroid hormone
Antithyroid Drugs • Therapies of hyperthyrosis include 131I radiotherapy, exairesis or medication. • Thiourea homologues are mainly used clinically. Iodine and iodide are used just in preparation for operations and thyroid crisis therapy. β receptor blockers can be used as adjunctive therapy for thyroid crisis.
硫脲类 • 硫氧嘧啶类: • 甲基硫氧嘧啶 • 丙基硫氧嘧啶 • 咪唑类 • 他巴唑(又称甲巯咪唑) • 甲亢平(又称卡比马唑)
Thiourea Physiological process • Absorption:Easy to be absorbed when taken orally. Thiouracil is the most fast to be absorbed. The bioavailability is 80% and the plasma protein binding rate is 75%. 20-30 min after administration , the drug turns to become effective with T1/2 of 2h. Imidazole is absorbed slowly. T1/2 of tapazole is 6h. • Distribution:Organs generally all over the body and can pass the placenta . The concentration in lacto is about 3 times as in blood . • Metabolism:Mainly in liver, fast . 60% are destroyed in vivo, the rest are eliminated by urine in a conjugative form. Carbimazole functions after turning into tapazole in vivo.
Thiourea Pharmacological actions • Inhibit peroxydase in adenocytes , which results in the inhibited oxydation of I- to I0 . Then , the iodation and couple of tyrosines can be stopped . So the biosynthesis of T3 and T4 is inhibited. But the effect occurs slowly as the iodine uptake and the hormone already synthesized are not effected. • Long time medication can lead to decrease of T3 and T4, which feedback increases the secretion of TSH and makes thyroid hyperplasy and hyperemic compensatorily. • Propylthiouracil can inhibit T4 turning to T3 and control T3 level in blood . So it is the first choice in hyperthyroidism crisis, severe hyperthyroidism and pregnant hyperthyroidism. • Inhibit immuno-system (as hyperthyroidism is related with abnormal immunoreactions).
Pathogenesis of Exophthalmos hyperthyroidism and function link of thiourea homologues • This disease is caused by an autoimmune IgG antibody LATS (long acting thyroid stimulator), which can bind to the receptors on thyroid adenocytes and stimulate oversecretion of thyroid hormones. • Thiourea homologues can not only inhibit synthesis of thyroid hormones, but also LATS in patients, which is a kind of immuno inhibition.
Thiourea Clinical application • Hyperthyroidism For who has mild symptoms and is not suitable to have operations and 131I radiotherapy. Give Larger dose at the beginning. After 1~3 months, symtoms decreased and basal metabolic rate returns to almost normal . Reduce to maintaining dose with a peroid of 1~2 years. Also can be used as adjunctive therapy of 131I radiotherapy. • Preparation before operation Medication before operation is good to decrease bleeding in operation and prevent thyroid crisis after operation. • Adjunctive medication of thyroid crisis Besides integrate measures, large dose of Thiourea homologues can be used as adjunctive therapy, So is Propranolol.
Comparison among common thiourea homologues drugs drug potencytherapeutic dose maintenance adverse effectsagranulemia (mg/d) dose incidence(%) incidence(%) mild moderate severe(mg/d) Methyl 1 200-300 400-600 13.8 0.5 thiouracil 300-400 50-100 Propyl 0.75 3.3 0.4 thiouracil Tapazole 10 20-30 40-60 7.1 0.1 Carbimazole10 30-40 5-10 1.9 0.8
Thiourea Adverse effects Although there are lots of adverse effects of thiourea homologues, incidences of propylthiouracil and tapazole are lower, 3% and 7%respectively. • Common adverse effects: Skin rash, headache, dinus, gastrointestinal uncomfortable , fatigue and so on. • Severe adverse effects: Bone marrow depression, agranulocytosis and so on. • Note: Periodic inspection of hemogram. The medication shoule be stopped if the symptoms as pharyngalgia, fever, cathaeresis occur. Thyroid cancer patients are forbidden to take.
Iodine and iodide Actions and applications • Low dose of iodine (physiological dose) could prevent and cure simple (endemicity) goiter. Add 1/10000~1/100000 potassium iodide or sodium iodide to salt could prevent the desease. • Large dose of iodine could inhibit the release of T3 and T4 (due to the inhibition of TG hydratase). • Used as adjunctive therapy for hyperthyroidism: ①preparation before operation: administration of aqueous iodine solution two weeks before operation degenerates the glandular tissue, decreases vessels and bleeding; ②adjunctive therapy for thyroid crisis: could be used combined with thiourea homologues.
Iodine and iodide Adverse effects and application notes • Acute effects: acute circumscribed edema,laryngeal edema and apnoea. • Chronic toxicity: mouth and throat burning sensation, increase secretion of salivary, eye irritation and so on. • Induce dysthyroid and hyperthyroidism after long medication. • Iodine could pass into the milk and through placenta, leading to neonat goiter. Pregnant and lactant women shoule take the drug with causious. • Allergic and active tuberculosis patients are forbidden to take.
Radioactive iodine(131I)T1/2 is 8.04 days Actions • 131I could be uptaken by throid , participate in the synthesis of T3, T4 and is stored in follecular colloid. • 131I mainly generatesβray (99%)with average and maximum path of 0.5mm and 2mm respectively. So the irradiation function is limited in the thyroid.It can destroy the glandular organ but can seldom destroy the surrounding tissues. • Γray generated by 131I accounts for 1% and can be detected in vitro. It is usually used in the examination of thyroid iodine uptaking function.
Radioactive iodine(131I) • Clinical application • Thyroid iodine uptake function examination: iodine uptake rate high when hyperthyroid, time of iodine uptake peak antelocation iodine uptake rate low when hypothyroid , time of iodine uptake peak retroposition • Hyperthyroidism • Trace amount could be used in diagnosis of thyroid functional status and thyroid adenoma .
Radioactive iodine Adverse effects and application notes • Hypothyroidism is the predominant complication. The adverse effects can be reduced by strict dose control and resisted by thyrine. • Patients with Total white blood cells less than 3000/mm3 are not suitable to take it. So are pragnant and lactant women, patients younger than 20 years old or with severe liver or kidney deseases.
receptor blockers • Valuable adjunctive therapy drugs for hyperthyroidism and thyroid crisis . They could improve symptoms caused by augmented sympathetic activity such as speed up heart rate and increase heart contraction force . They can also reduce the thyroid hormone secretion and T3 synthesis by inhibiting 5`-deiodinase . • Control hyperthyroidism symptoms and can be used in preparation before operation .
receptor blockers • Clinical application • Adjunctive therapy for hyperthyroidism and hyperthyroidism crisis. • Mechanism of pharmacological actions • Excited sympathetic-adrenergic system β1 receptor blockage—heart rate drop Central β receptor blockage —to reduce anxiety β2 receptor on NA energinic peripheral nerve endings presynaptic membrane blockage reduces the release of NA. • Appropriately reduce T3, T4 secretion.