Download
1 / 42
430 likes | 582 Views
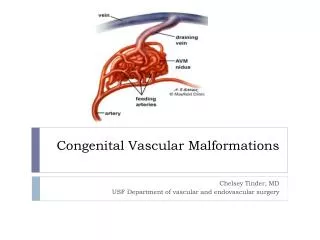
Learn about the complexities of congenital clubfoot, its causes, diagnosis, and treatment options to help affected children lead a better quality of life. Discover the adaptive changes, abnormal foot relations, and characteristics of this condition to make informed decisions.

E N D
Congenital Clubfoot (Congenital Talipes Equino-Varus) dr n. med. Dariusz Mątewski
THE NORMAL FOOT Complex organ that is required to be • Stable:for supporting the body weight during standing • Resilient: for walking and running • Mobile:to accommodate variations of surface • Cosmetic
FOOT ABNORMALITIES Definitions Talipes: Talus = ankle Pes = foot Equinus:(Latin = horse) Foot that is in a position of plantar flexion at the ankle, Calcaneus:Full dorsiflexion at the ankle
FOOT ABNORMALITIES Planus: flatfoot Cavus:highly arched foot Varus: heel going towards the midline Valgus:heel going away from the midline Adduction:forefoot going towards the midline Abduction:forefoot going away From the midline Forefoot Hind foot
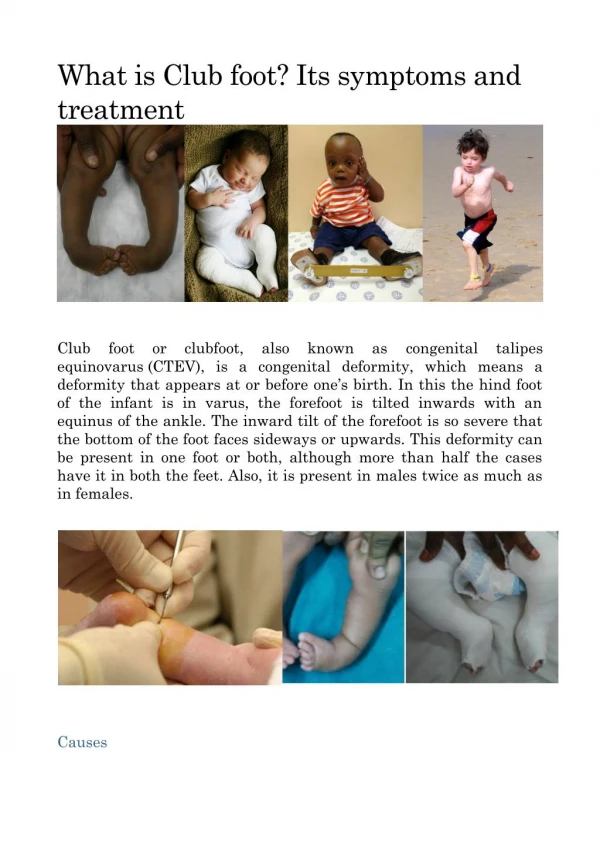
CONGENITAL CLUBFOOT Substantial deformity of the foot, which gives its stunted lumpy appearance In the full-blown equinovarus deformity the heel is in equinus, the entire hindfoot in varus and the mid and forefoot adducted and supinated.
CONGENITAL TALIPES Types Postural : Equino-VarusCalcaneo-Valgus Minor and correctable Look for DDH
CONGENITAL CLUBFOOT Types Idiopathic: Teratologic: Acquired, Secondary to : • CNS Disease : Spina bifida, Poliomyelitis • Arthrogryposis • BoneDefect : fibula / tibia
CONGENITAL CLUBFOOT Congenital clubfoot (CTEV) occurs typically in an otherwise normal child.
CONGENITAL CLUBFOOT Etiology • Multifactorial • Polygenic although many of these factors are speculative
CONGENITAL CLUBFOOT Etiology Some of these factors are : • Histologic anomalies in connective tissue • Abnormal muscle and tendon insertions • Vascular anomalies • Abnormal intrauterine forces • Germ defects • Arrested fetal development
CONGENITAL CLUBFOOT Incidence • Occurs approximately in 1-2 of every 1000 live birth • In affected families, clubfeet are about 30 times more frequent in offspring • Male are affected in about 65% of cases • Bilateral cases are as high as 30 – 40 %
CONGENITAL CLUBFOOT Geographic Distribution • White race (caucasian) • Mediterranean Coast & North Africa
CONGENITAL CLUBFOOT Basic Pathology • Abnormal Tarsal Relation Congenital Dislocation / Subluxation Talo Calcaneo Navicular Joint • Soft Tissue Contracture Congenital Atresia EGG & CHICKEN
CONGENITAL CLUBFOOT • The neck of the talus points downwards and deviates medially. • The posterior part of the calcaneum is held close to the fibula by a tight calcaneo-fibular ligament, and is tilted into equinus and varus; • The navicular and entire forefoot are shifted medially and rotated into supination (the composite varus deformity).
CONGENITAL CLUBFOOT Adaptive Changes Wolff’s Law “ Every change in the use of static function of bone caused a change in the internal form or architecture as well as alteration in its external formation and function according to mechanical law ” Davis Law “ When ligaments and soft tissue are in loose or lax state; they gradually shorten ”
CONGENITAL CLUBFOOT Adaptive Changes • Bony : Change in the shape of tarsal and metatarsal bones especially after walking • Soft Tissue : Shortening ? Contracture in the Concave Side 1- Muscles 2- Tendons 3- Ligaments 4- Joints Capsule 5- Skin 6- Nerves & Vessels
CONGENITAL CLUBFOOT Diagnosis General Examination : Exclude • Neurological lesion that can cause the deformity “Spina Bifida” • Other abnormalities that can explain the deformity “Arthrogryposis, Myelodysplasia” • Presence of concomitant congenital anomalies “Proximal femoral focal deficiency” • Syndromatic clubfoot “Larsen’s syndrome, Amniotic band Syndrome”
CONGENITAL CLUBFOOT Diagnosis Spina Bifida = Paralytic TEV
CONGENITAL CLUBFOOT Diagnosis Characteristic Deformity : Hindfoot • Equinus (Ankle joint) • Varus (Subtalar joint) Forefoot • Supination (Forefoot) • Adduction(Lisfranc joint) • Cavus
CONGENITAL CLUBFOOT Diagnosis the foot is both turned and twisted inwards so that the sole faces posteromedially.
CONGENITAL CLUBFOOT Diagnosis Hindfoot Forefoot Equinus, Varus Adduction, Supination, Cavus the ankle is in equinus, the heel is inverted and the forefoot is adducted and supinated
CONGENITAL CLUBFOOT Diagnosis
CONGENITAL CLUBFOOT Diagnosis • Short Achilles tendon • High and small heel • No creases behind heel • Abnormal crease in middle of the foot • Foot is smaller in unilateral affection • Callosities at abnormal pressure areas • Internal torsion of the leg • Calf muscles wasting • Deformities don’t prevent walking
CONGENITAL CLUBFOOT Diagnosis
CONGENITAL CLUBFOOT Diagnosis X-Rayneeded to assess progress of treatment
CONGENITAL CLUBFOOT Treatment The goal of treatment of clubfoot is to obtain a plantigrade foot that is functional, painless, and stable over time A cosmetically pleasing appearance is also an important goal sought by the surgeon and the family
CONGENITAL CLUBFOOT Treatment Non surgical treatment should begin shortly after birth • Gentle manipulation • Immobilization - Strapping ???? - POP or synthetic cast
CONGENITAL CLUBFOOT Treatment Non surgical treatment should begin shortly after birth • Gentle manipulation • Immobilization - Strapping ???? - POP or synthetic cast
CONGENITAL CLUBFOOT Treatment Non surgical treatment should begin shortly after birth • Splints to maintain correction - Dennis Brown splint - Ankle-foot orthosis ????
CONGENITAL CLUBFOOT Treatment Manipulation and serial casts • Validity, up to 6 months ! • Technique “Ponseti” • Avoid false correction • When to stop ? • Maintaining the correction • Follow up to watch and avoid recurrence
CONGENITAL CLUBFOOT Treatment Ponseti technique • Always use long leg casts, change weekly. • First manipulation raises the 1st metatarsal to decrease the cavus • All subsequent manipulations include pure abduction of forefoot with counter-pressure on neck of talus. • Never pronate ! • Never put counter pressure on calcaneus or cuboid.
CONGENITAL CLUBFOOT Treatment Ponseti technique (cont.) • Cast until there is about 60 degrees of external rotation (about 4-6 casts) • Percutaneous tendo Achilles tenotomy in cast room under local anesthesia, followed by final cast (3 weeks) • After final cast removal, apply Normal last shoes with Denis Browne bar set at 70 degrees external rotation (40 degrees on normal side) • Denis Browne splint full time for two months, then night time only for two-four years. • 35% need Anterior Tibialis tendon transfer at age 2-3
CONGENITAL CLUBFOOT Surgical Treatment Indications • Late presentation, after 6 months of age ! • Complementary to conservative treatment • Failure of conservative treatment • Residual deformities after conservative treatment • Recurrence after conservative treatment
CONGENITAL CLUBFOOT Surgical Treatment • Types (soft tissue and bony operations) • Time of surgery • Selection of the procedure and the incision • Post operative care • Follow up • Complications
CONGENITAL CLUBFOOT Surgical Treatment Soft tissue operations • Release of contractures • Tenotomy • Tendon elongation • Tendon transfer • Restoration of normal bony relationship
CONGENITAL CLUBFOOT Surgical Treatment
CONGENITAL CLUBFOOT Surgical Treatment
CONGENITAL CLUBFOOT Surgical Treatment Bony operations • Indications • Usually accompanied with soft tissue operation • Types: - Osteotomy, to correct foot deformity or int. tibial torsion - Wedge excision - Arthrodesis (usually after bone maturity) one or several joints - Salvage operation to restore shape
CONGENITAL CLUBFOOT Surgical Treatment
CONGENITAL CLUBFOOT Surgical Treatment