Download
1 / 64
650 likes | 675 Views
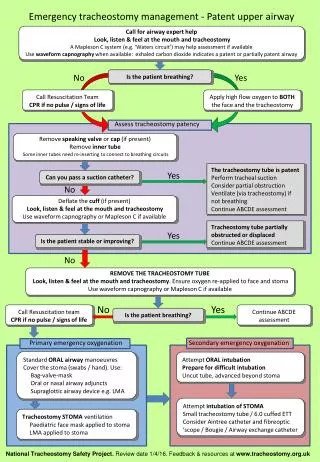
Emergency Airway Management ________________________________ Mark L. Freedman MD, FRCP. Objectives. To review the indications for intubation To briefly discuss RSI To review the airway assessment To discuss difficult airways To review difficult airway algorithms

E N D
Emergency Airway Management ________________________________ Mark L. Freedman MD, FRCP
Objectives • To review the indications for intubation • To briefly discuss RSI • To review the airway assessment • To discuss difficult airways • To review difficult airway algorithms • To discuss an approach to difficult airways • Case discussions
Case • 13 yr/o M mountain biking • Neck vs. handlebars • Sitting-up on bike path • Anterior neck swelling • VSS • Mild stridor • What will you do?
The 4 Questions • Does this patient need intubation now? • Is this a crash situation? • Is this a difficult airway? 4. Can I use RSI?
Outline • Indications for intubation • Basic airway algorithm • Difficult airways • Difficult airway algorithm • Securing the difficult airway • Cases
Outline • Indications for intubation • Basic airway algorithm • Difficult airways • Difficult airway algorithm • Securing the difficult airway • Cases
Indications for Intubation • Failure of oxygenation • Failure of ventilation • Failure to protect • Impending obstruction • Expected management
Failure of Oxygenation • Low FiO2 • Failure of ventilation • V/Q mismatch • Diffusion abnormalities • Anemia • Low C.O. • Increased tissue O2 consumption
Failure of Ventilation Brain; CHI Stroke Raised ICP Stem; Stroke Narcotics Injury Cord; SCI Degenerative diseases Nerve; Peripheral Neuropathy NMJ; Myasthenia gravis Guillon-Barre NMJBs Muscle; Myopathy Thorax; Burn eschar Rib fractures Lungs; Restrictive disease Contusions Abdomen; Tense ascities Compartment Syndrome
Failure to Protect • Low or dropping GCS • “GCS less than 8, intubate” • Aspiration risk
Impending Obstruction • Expanding hematoma • Deep space infection • Epiglotitis/Bacterial tracheitis • Angioedema/Allergic reaction • Inhalation injury • Eschar • Foreign body • Tumour • Others….
Outline • Indications for intubation • Basic airway algorithm • Difficult airways • Difficult airway algorithm • Securing the difficult airway • Cases
Basic airway algorithm Yes Fails Crashing ? Crash Airway No Yes Fails Difficult Airway ? Difficult Airway Failed Airway No Fails RSI ?
The 8 “P”s of RSI • 0 - 10min Preparation • 0 - 5 min Preoxygenation • 0 – 3 min Premedication • 0 Pharmacological Induction • 0 Pressure • 0 Paralysis • 0 + 45 sec Place tube • 0 + 1 min Post Intubation Care
Outline • Indications for intubation • Basic airway algorithm • Difficult airways • Difficult airway algorithm • Securing the difficult airway • Cases
Difficult Airways • Difficult mask ventilation • Difficult laryngoscopy • Difficult tracheal intubation • Combinations of above
Difficult Airway • EMS Incidence; • Not known • ED Incidence; • Not known • Cricothyrotomy reported as high as 1% • Definitely inflated • Reflects an aggressive approach without employing alternate intubation techniques
Difficult Airways • Difficult mask ventilation; • Predicting the difficulty (BOOTS); • Bearded • Older (> 55 years) • Obese (BMI > 26 kg/m2) • Toothless • Snores
Difficult Airways • Difficult laryngoscopy/intubation; • Predicting the difficulty (LEMON); • Look • Evaluate; 3,3,2 • Mallampati score • Obstruction • Neck mobility
Difficult Airways • The airway assessment; • Look (BOOTS, others) • Evaluate; 3,3,2 • Mallampati score • Obstruction • Neck mobility
Difficult Airways • Specific situations; • Trauma • Obesity • Pregnancy • Pediatrics
Difficult Airways • Not a catastrophe if you can’t see well • Not even if you can’t intubate • But, if you ALSO can’t ventilate…….
Outline • Indications for intubation • Basic airway algorithm • Difficult airways • Difficult airway algorithm • Securing the difficult airway • Cases
Difficult Airway Anticipated Unanticipated Fail to Intubate Cooperative Time Uncooperative No time + Ventilation Sats Maintained - Ventilation Sats Dropping OR? Topicalize Sedate Awake; Laryngoscope Glidescope Lighted Stylet FOB Help Sedate Topicalize “Brutane” Sedate More RSI+Double set-up Better Position BURP Better Blade Better Drugs Bougie Better Person Glidescope Bronch BNTI LMA TTJV Cricothyrotomy TTJV Cricothyrotomy * Suction if bleeding *
Outline • Indications for intubation • Basic airway algorithm • Difficult airways • Difficult airway algorithm • Securing the difficult airway • Cases
Securing the Difficult Airway • Anticipated; • Best to get patient to ED/OR • BVM as bridge • Otherwise intubation • Don’t burn bridges
Securing the Difficult Airway • Unanticipated; • Can you ventilate?? • Yes = time • No = trouble
Difficult Airway Anticipated Unanticipated Fail to Intubate Cooperative Time Uncooperative No time + Ventilation Sats Maintained - Ventilation Sats Dropping Help Sedate Topicalize “Brutane” Sedate More RSI+Double set-up Transport Observe Better Position BURP Better Blade Better Drugs Bougie Better Person Glidescope Bronch BNTI LMA TTJV Cricothyrotomy TTJV Cricothyrotomy * Suction if bleeding *
Difficult Airways • Difficult ventilation; 1. Head tilt/chin lift 2. Exaggerated Jaw thrust 3. Oral/nasal airways 4. Two handed/two person technique 5. Consider mask change 6. Ease up on cricoid pressure 7. Rule out FB
Difficult Airway Anticipated Unanticipated Fail to Intubate Cooperative Time Uncooperative No time + Ventilation Sats Maintained - Ventilation Sats Dropping Help Sedate Topicalize “Brutane” Sedate More RSI+Double set-up Transport Observe Better Position BURP Better Blade Better Drugs Bougie Better Person Glidescope Bronch BNTI LMA TTJV Cricothyrotomy TTJV Cricothyrotomy * Suction if bleeding *