Download

1 / 59
740 likes | 1.4k Views
Traumatic Injuries, Cracked Teeth and vertical root fractures (VRF). Fact. Most dental trauma occurs in 7_12 age range And most trauma occurs in the anterior region of the mouth, maxilla>mandible. 1. Crown FX without Pulp exposure. NO PROBLEM, RELAX AND RESTORE.

E N D
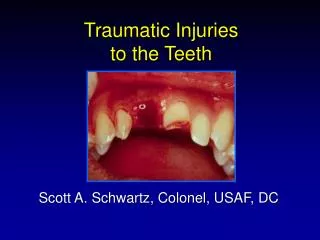
Traumatic Injuries, Cracked Teeth and vertical root fractures (VRF)
Fact • Most dental trauma occurs in 7_12 age range • And most trauma occurs in the anterior region of the mouth, maxilla>mandible
1. Crown FX without Pulp exposure NO PROBLEM, RELAX AND RESTORE
Complicated Crown FX with Pulp Exposure @80% IF w/in 24hrs Partial Pulpotomy@95% Full pulpotomy @75% OR: EXTIRPATION if root is fully formed Pulp Cap?
2. Crown-Root Fracturesometimes fractures at an angle Angular Fracture: Is this restorable?
Remember, • In all trauma, the primary purpose of our treatment is to keep the pulp vital, if at all possible, ESPECIALLY if apex is open • WHY?
Apexogenesis vs ApexificationDealing with the immature root Apexogenesis (Vital Pulp) best to treat w pulpotomy. The idea is to allow the vital pulp to remain vital and complete the development of the root apex as well as thickening of the RC walls RCT maybe needed later BUT not if tooth remains asymptomatic AND vital Apexification (Necrotic Pulp) Hoping to get closure of the apex (&there is NO wall thickening)to be able to later do a proper RC seal via obturation. CaOH + time is proper tx over 3-18mo RCT ALWAYS NEEDED HERE* and is less predictable due to thinner walls Objectof either treatment is to allow for roofing over of apex and allow RCT to be done at a later date.
And now, Regeneration? • Revascularization of immature permanent teeth utilizing a mixture of antibiotics(3 weeks), creating a blood clot w/in the RCS which produces development of the tooth structure
Root FX (Horizontal) What do you do here? Try to reposition and splint 2-4 wks, check for vitality q 30 days
4. Luxation Injuries(MOST COMMON OF ALL DENTAL INJURIES)30-44% • Concussion • Subluxation • Extrusion • Lateral • Intrusion WORST CASE SEQUELAE? PULP NECROSIS EXTERNAL/INTERNAL ROOT RESORPTION Possible tooth loss AVULSION
Concussion Luxation Injury • Least severe of Luxation injuries • No displacement of tooth nor excessive mobility • Tooth tender to touch “Bruised PDL” • No radiographic abnormalities • Assess vitality in 4 wks
Subluxation Luxation Injury • Tooth tender to touch & slightly mobile (1+) but not displaced • Possible hemorrhage from gingival crevice • No radiographic abnormalities • Damage to supporting structures? • Assess vitality in 4 weeks
Extrusion Luxation Injury • Elongated mobile tooth • Cl. II mobility or greater • Radiographs show increased apical periodontal space • Manually reposition • Reposition tooth + Flexible splint (2 weeks) • Assess vitality in 4 weeks
What is a flexible splint? -Allows physiologic movement of the teeth in order to minimize ankylosis -In the past, .028 gauge ortho wire bonded to tooth for 7-10 days unless alveolar FX had occurred. Then 4-8 wks OR: 4-6# fishing line bonded to teeth -Currently, titanium trauma splint (TTS) is recommended
Semi-rigid or flexible splinting • Experimental studies in non-human primates have demonstrated that rigid splinting ,especially for prolonged periods, leads to ankylosis &/or external resorption. • Maintaining a slight degree of tooth mobility appears to be beneficial to PDL healing
Titanium Trauma Splint Medaris AG, Basel Switzerland
TTS splint • Insert picture of same • Splinting of traumatized teeth with a new device:TTS (Titanium Trauma Splint) • Medartis AG, Basel, Switzerland • Von arx T, etal Dent Traumatol, ’01;17:180-84
Lateral Luxation Injury • Displaced laterally & often locked in bone • Not tender to touch, not mobile • Alveolus fractured • Percussion test: high metallic sound (ankylosis) • Increased PDL space best seen on eccentric or occlusal radiographs • Anesthetize & reposition + Flexible splint (4 weeks) • Assess vitality in 4 weeks
Intrusion Luxation InjuryExternal root resorption likely • Most severe of luxations*** • Tooth appears shorter: displaced into alveolar bone • PDL destruction/alveolar crushing) Beware of ankylosis/resorption/ • pulp necrosis is all but certain in mature teeth*** • Not tender to touch, not mobile • Percussion test: high metallic sound • Radiographs not always conclusive • Slightly luxate with forceps or band and move orthodontically. • Splinting is not usually necessary (>4 weeks) • Tooth with open apex may spontaneously re-erupt.
Treatment of intrusion luxation • Closed apex needs ortho. or surgical repositioning and probable RCT in 1-3 weeks In all LUXATION and especially INTRUSION injuries, the apical neurovascular bundle and attachment apparatus will be affected to some degree>>>loss of vitality & internal/external resorption
5. Avulsion • Tooth is knocked completely out of mouth • Viability of the PDL must be preserved for success • Extra-oral dry time is CRITICAL 30-60”*** • Must be replaced in socket ASAP (15-20”) in order to.. • Prevent ankylosis • Prevent external root resorption To replant or not? should be “decent tooth”: No point in replanting THIS one
Replant? • TX is aimed at minimizing the inflammation from the two main consequences of avulsion, namely; attachment damage and pulpal infection that inevitably results • The SINGLE most VIP factor in achieving a favorable outcome is the SPEED at which a clean tooth is properly replanted • Keeping the attached PDL moist is VIP!!*
Replantation guidelines HOW FAST IS FAST? 5”, 30” 60”, TAKE YOUR PICK, it depends on whose book you read! • If tooth is out of the mouth less than 15-20”, replant according to guidelines • If tooth was out and placed in cold milk or other physiological solution w/in 15-20” & available for replantation w/in 30”, replant and follow guidelines • If tooth is out > 60” and not stored, there is usually one outcome: resorption and probable loss • If the pt is pre adolescent, the tooth may become infraoccluded (ankylosed) as he/she grows older
To replant or not • If the root of the avulsed tooth is not completely formed, the prognosis for survival and revascularization is possible if not left out>60” • If root is incompletely formed and replantation is rapid, vitality may be maintained but is not predictable
First Aid Instructions • Handle by crown only • Pick off debris with tweezers • Replant tooth if possible • _________________________________ • If not, transport in appropriate medium: • “HBSS (Hank’s Balanced Salt solution) • OR “Via Span” (if available) • OR milk if above not available • OR place in vestibule (saliva) & Report to dental office ASAP
Once in Dental office: • Take films to make sure there is no alveolar FX & that adjacent teeth are OK • “Save-a-tooth” (Hank’s Balanced Salt solution) • OR “Via Span”, milk, saline • Gently clean socket • Replant and check occlusion • Splint (7-10 days) • RX antibiotics
Avulsion InjuryWhat NOT to do! • Do Not • Handle by root • Scrub root • Allow tooth to dry • Submerge the tooth in water (tap water is hypotonic> and will cause cell rupture) AAE has a Flow Chart Outlining Current Treatment Management Protocols of both Luxation and Avulsion cases ..www.aae.org.
If over 60” “dry time” • Remove remnants ofPDL by soaking in acid for 1” • Soak in Stannous Fl for 5” • No harm done to go ahead and complete endo ASAP • Splint
Immature Tooth: Open Apex, revascularization is possible if out less than 30-60” • Replant as above EXCEPT different • Soak tooth in Doxycycline (1mg/20cc saline)<replantation for 5” • Monitor pulp vitality closely (q 30 d or until root development is confirmed) • Vital Open apex will NOT necessarily require RCT UNLESS pulp becomes necrotic. • What if it does? Do we do apexogenesis then?
Ankylosis • A problem following trauma and long termrigid splinting • Tooth is solidly fixed and has a high metallic ring when percussing. Does not erupt with other teeth • May lead to massive external resorption & loss of tooth • Internal= appearance of “aneurysm” w/in canal.
Complications with Replanted avulsed teeth & Possibly with Rigid Long-Term Splinting • Ankylosis (Replacement Resorption)
Vertical Root Fracture Look for ‘J’-Shaped apical lesion Look for Drop-off Pocket if . . . . VRF difficult to confirm radiographically –UNLESS separation of segments occurs
Other methods of discovering VERTICAL ROOT FRACTURE A surgical exploration is usually the only other way to confirm presence of VRF* Transillumination Restoration Removal + Staining
Flare-ups • A flare-up is an acute exacerbation of an asymptomatic pulp/or periapicalpathosis after the initiation or continuation of root canal treatment.
Patient Presentation • Pain • Pain and swelling
Factors • Mechanical • chemical • Emotional state • Gender • Microbial • Immunological • Psychological state • Regulation of periapical inflammation
Incidence • 1.4 to 19% • 20 to 40%
Age of Patient? • There is a lack of agreement concerning the influence of age on the incidence of flare-up. • 40_59 year(most) • Under the age of 20(least)
Gender and Flare-ups • Women(most)
Systemic conditions • Host resistance • Allergy
Anatomic Location • Mandibular teeth • premolars