Download
1 / 1
10 likes | 91 Views
974. The Effects of HIV-1 Viral Suppression and Non-Viral Factors on Clinically Significant Proteinuria in the HAART Era Samir Gupta, Nora Franceschini, Lynda Szczech, Marlene Smurzynski, Robert Kalayjian, and the ACTG ALLRT Study Team. Contact Information SK Gupta, MD, MS

E N D
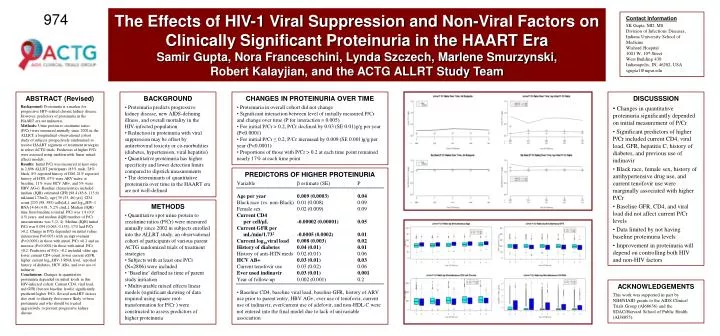
974 The Effects of HIV-1 Viral Suppression and Non-Viral Factors on Clinically Significant Proteinuria in the HAART Era Samir Gupta, Nora Franceschini, Lynda Szczech, Marlene Smurzynski, Robert Kalayjian, and the ACTG ALLRT Study Team Contact Information SK Gupta, MD, MS Division of Infectious Diseases, Indiana University School of Medicine Wishard Hospital 1001 W. 10th Street West Building 430 Indianapolis, IN, 46202, USA sgupta1@iupui.edu ABSTRACT (Revised) Background: Proteinuria is a marker for progressive HIV-related chronic kidney disease. However, predictors of proteinuria in the HAART era are unknown. Methods: Urine protein to creatinine ratios (P/Cr) were measured annually since 2002 in the ALLRT, a longitudinal observational cohort study of subjects prospectively randomized to receive HAART regimens or treatment strategies in select ACTG trials. Predictors of higher P/Cr were assessed using multivariable linear mixed effects models. Results: Initial P/Cr was measured at least once in 2,806 ALLRT participants (83% male, 28% black, 8% reported history of DM, 21% reported history of HTN, 67% were ARV-naïve at baseline, 11% were HCV AB+, and 5% were HBV AG+). Baseline characteristics included median (IQR) estimated GFR [98.4 (85.6, 115.6) mL/min/1.73m2], age [39 (33, 46) yrs], CD4 count [233 (98, 385) cells/µL], and log10HIV-1 RNA [4.64 (4.01, 5.27) c/mL]. Median (IQR) time from baseline to initial P/Cr was 1.9 (0.9, 4.5) years, and median (IQR) number of P/Cr measurements was 3 (2, 4). Median (IQR) initial P/Cr was 0.094 (0.063, 0.155); 17% had P/Cr >0.2. Change in P/Cr depended on initial values (interaction P=0.005) with an improvement (P<0.0001) in those with initial P/Cr >0.2 and an increase (P<0.0001) in those with initial P/Cr ≤0.2. Predictors of P/Cr >0.2 included older age, lower current CD4 count, lower current eGFR, higher current log10HIV-1 RNA level, reported history of diabetes, HCV AB+, and ever use of indinavir. Conclusions: Changes in quantitative proteinuria depended on initial levels in this HIV-infected cohort. Current CD4, viral load, and GFR (but not baseline levels) significantly predicted higher P/Cr. Several non-HIV factors also exist to identify those more likely to have proteinuria and who should be treated aggressively to prevent progressive kidney disease. • BACKGROUND • Proteinuria predicts progressive kidney disease, new AIDS-defining illness, and overall mortality in the HIV-infected population • Reduction in proteinuria with viral suppression may be offset by antiretroviral toxicity or co-morbidities (diabetes, hypertension, viral hepatitis) • Quantitative proteinuria has higher specificity and lower detection limits compared to dipstick measurements • The determinants of quantitative proteinuria over time in the HAART era are not well-defined • CHANGES IN PROTEINURIA OVER TIME • Proteinuria in overall cohort did not change • Significant interaction between level of initially measured P/Cr and change over time (P for interaction = 0.005) • For initial P/Cr > 0.2, P/Cr declined by 0.03 (SE 0.01)g/g per year (P<0.0001) • For initial P/Cr ≤ 0.2, P/Cr increased by 0.009 (SE 0.001)g/g per year (P<0.0001) • Proportions of those with P/Cr > 0.2 at each time point remained nearly 17% at each time point • DISCUSSSION • Changes in quantitative proteinuria significantly depended on initial measurement of P/Cr • Significant predictors of higher P/Cr included current CD4, viral load, GFR, hepatitis C, history of diabetes, and previous use of indinavir • Black race, female sex, history of antihypertensive drug use, and current tenofovir use were marginally associated with higher P/Cr • Baseline GFR, CD4, and viral load did not affect current P/Cr levels • Data limited by not having baseline proteinuria levels • Improvement in proteinuria will depend on controlling both HIV and non-HIV factors • PREDICTORS OF HIGHER PROTEINURIA • Variable β estimate (SE) P • Age per year 0.009 (0.0003) 0.04 • Black race (vs. non-Black) 0.01 (0.008) 0.09 • Female sex 0.02 (0.009) 0.09 • Current CD4 • per cell/µL -0.00002 (0.00001) 0.05 • Current GFR per • mL/min/1.732 -0.0005 (0.0002) 0.01 • Current log10viral load 0.008 (0.003) 0.02 • History of diabetes 0.04 (0.01) 0.01 • History of anti-HTN meds 0.02 (0.01) 0.06 • HCV AB+ 0.03 (0.01) 0.03 • Current tenofovir use 0.03 (0.02) 0.06 • Ever used indinavir 0.03 (0.01) 0.001 • Year of follow-up 0.002 (0.001) 0.2 • Baseline CD4, baseline viral load, baseline GFR, history of ARV use prior to parent entry, HBV AG+, ever use of tenofovir, current use of indinavir, ever/current use of adefovir, and non-HDL-C were not entered into the final model due to lack of univariable association • METHODS • Quantitative spot urine protein to creatinine ratios (P/Cr) were measured annually since 2002 in subjects enrolled into the ALLRT study, an observational cohort of participants of various parent ACTG randomized trials of treatment strategies • Subjects with at least one P/Cr (N=2806) were included • ‘Baseline’ defined as time of parent study initiation • Multivariable mixed effects linear models (significant skewing of data required using square root-transformation for P/Cr ) were constructed to assess predictors of higher proteinuria ACKNOWLEDGEMENTS This work was supported in part by NIH/NIAID grants to the AIDS Clinical Trials Group (AI68636) and the SDAC/Harvard School of Public Health (AI38855).