Download
1 / 1

E N D
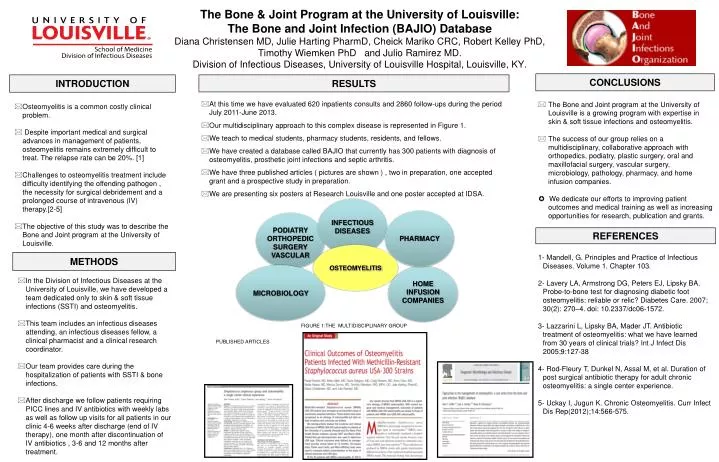
The Bone & Joint Program at the University of Louisville:The Bone and Joint Infection (BAJIO) DatabaseDiana Christensen MD, Julie Harting PharmD, Cheick Mariko CRC, Robert Kelley PhD, Timothy Wiemken PhD and Julio Ramirez MD. Division of Infectious Diseases, University of Louisville Hospital, Louisville, KY. CONCLUSIONS INTRODUCTION RESULTS • The Bone and Joint program at the University of Louisville is a growing program with expertise in skin & soft tissue infections and osteomyelitis. • The success of our group relies on a multidisciplinary, collaborative approach with orthopedics, podiatry, plastic surgery, oral and maxillofacial surgery, vascular surgery, microbiology, pathology, pharmacy, and home infusion companies. • ✪ We dedicate our efforts to improving patientoutcomes and medical training as well as increasing opportunities for research, publication and grants. • Osteomyelitis is a common costly clinical problem. • Despite important medical and surgical advances in management of patients, osteomyelitis remains extremely difficult to treat. The relapse rate can be 20%. [1] • Challenges to osteomyelitis treatment include difficulty identifying the offending pathogen , the necessity for surgical debridement and a prolonged course of intravenous (IV) therapy.[2-5] • The objective of this study was to describe the Bone and Joint program at the University of Louisville. • At this time we have evaluated 620 inpatients consults and 2860 follow-ups during the period July 2011-June 2013. • Our multidisciplinary approach to this complex disease is represented in Figure 1. • We teach to medical students, pharmacy students, residents, and fellows. • We have created a database called BAJIO that currently has 300 patients with diagnosis of osteomyelitis, prosthetic joint infections and septic arthritis. • We have three published articles ( pictures are shown ) , two in preparation, one accepted grant and a prospective study in preparation. • We are presenting six posters at Research Louisville and one poster accepted at IDSA. INFECTIOUS DISEASES PHARMACY PODIATRY ORTHOPEDIC SURGERY VASCULAR REFERENCES OSTEOMYELITIS METHODS • 1- Mandell, G. Principles and Practice of Infectious Diseases. Volume 1. Chapter 103. • 2- Lavery LA, Armstrong DG, Peters EJ, Lipsky BA. Probe-to-bone test for diagnosing diabetic foot osteomyelitis: reliable or relic? Diabetes Care. 2007; 30(2): 270–4. doi: 10.2337/dc06-1572. • 3- Lazzarini L, Lipsky BA, Mader JT. Antibiotic treatment of osteomyelitis: what we have learned from 30 years of clinical trials? Int J Infect Dis 2005;9:127-38 • 4- Rod-Fleury T, Dunkel N, Assal M, et al. Duration of post surgical antibiotic therapy for adult chronic osteomyelitis: a single center experience. • 5- Uckay I, Jugun K. Chronic Osteomyelitis. Curr Infect Dis Rep(2012);14:566-575. MICROBIOLOGY HOME INFUSION COMPANIES • In the Division of Infectious Diseases at the University of Louisville, we have developed a team dedicated only to skin & soft tissue infections (SSTI) and osteomyelitis. • This team includes an infectious diseases attending, an infectious diseases fellow, a clinical pharmacist and a clinical research coordinator. • Our team provides care during the hospitalization of patients with SSTI & bone infections. • After discharge we follow patients requiring PICC lines and IV antibiotics with weekly labs as well as follow up visits for all patients in our clinic 4-6 weeks after discharge (end of IV therapy), one month after discontinuation of IV antibiotics , 3-6 and 12 months after treatment. FIGURE 1:THE MULTIDISCIPLINARY GROUP PUBLISHED ARTICLES