Download
1 / 24
240 likes | 250 Views
This training course, led by Dr. Gerry McCartney, Head of Public Health Observatory Division at NHS Health Scotland, explores the complexities of interpreting numbers in public health. Topics covered include causality, attributable fractions, pitfalls in screening, and more. Learn how to analyze data effectively and understand the implications for population health.

E N D
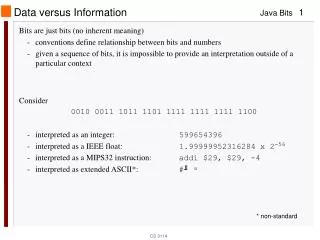
Interpreting numbers – more tricky bits ScotPHO training course March 2011 Dr Gerry McCartney Head of Public Health Observatory Division NHS Health Scotland gmccartney@nhs.net
Content • More on causality • Attributable fractions • Screening – pitfalls to watch out for
Does A cause B? A B A B A C B A ? B
Factors which make causality more likely Bradford-Hill criteria • Strength of association • Consistency • Specificity • Temporality • Biological gradient • Plausibility • Coherence • Experiment • Analogy
Does coffee cause ischaemic heart disease? Coffee Ischaemic heart disease
Effect modifiers • Factors that do not lie on the causal pathway but which influence the magnitude of effect Male gender (effect modifier) Smoking Ischaemic heart disease
Necessary or sufficient causes? Asbestos exposure Asbestosis Smoking Lung cancer Jumping from plane without parachute Squished onto ground
Attributable fractions/risk • “What fraction of disease incidence in the exposed group is attributable to the risk factor?” • Calculated by taking the relative risk in an unexposed group from the relative risk in an exposed group
Attributable fractions/risk Attributable fractions can also be applied to the whole population using the formula: = (risk in total population – risk in unexposed population) / risk in total population
Screening • Why do we screen for conditions? • When is screening appropriate? • Problems with evaluation of screening programmes • Particular biases
Why screen for conditions? • To improve outcomes for individuals • Keep Well health checks • Breast mammography • To improve outcomes for populations • Port health checks • Employment checks
When should you screen? Based on the Wilson – Junger criteria: • Is there an effective intervention? • Does earlier intervention improve outcomes? • Is there a screening test which recognises disease earlier than usual? • Is the test available and acceptable to the target population? • Is the disease a priority? • Do the benefits outweigh the costs?
Screening – why is it different? • Individuals may not benefit • Involves people who are well subjecting themselves to testing – medicalisation • Creation of a pre-disease state • False positive tests • False negative tests • Initiated by health professionals not individuals • Cost-benefit depends on prevalence within a population • Inequalities implications
Particular biases • Lead time bias • Given that screening picks up disease at an earlier stage – the time between diagnosis and death increases without any actual increase in survival Symptoms Death Death Detected by screening
Length time bias • Screening is more likely to detect less aggressive disease and therefore can give impression of improved survival X X X X X X X
Measures used in screening • Sensitivity is the likelihood that those with disease will be picked up by the screening test • Specificity is the likelihood that those with a negative screening test will not have the disease • Positive predictive value is the likelihood that those with a positive test will have the disease • Negative predictive value is the likelihood that those with a negative test will not have the disease
Measures for screening • Sensitivity and Specificity • Positive predictive value and Negative predictive value
Measures for screening • Sensitivity and Specificity • Positive predictive value and Negative predictive value Sensitivity = 300/320 = 94% Specificity = 3000/3030 = 99% PPV = 300/330 = 91% NPV = 3000/3020 = 99%
Summary • Bradford-Hill criteria can be used to judge whether an association is likely to be causal • Attributable fractions can help identify the discrete contribution of particular risks to an outcome • Screening is different to other medical interventions and can cause harm • Screening evaluations have their own potential biases – lead time and length time bias
Questions gmccartney@nhs.net