Download
1 / 40
410 likes | 550 Views
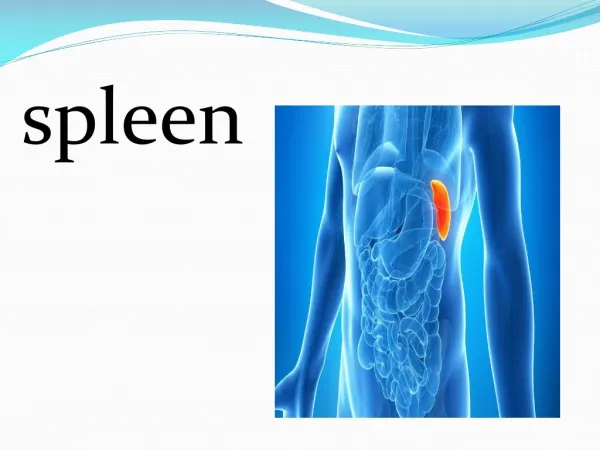
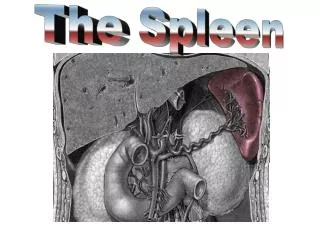
SPLEEN. I. Anatomy - weight – approximately 100-150 grams - located in the left upper and protected by the lower portion of the rib cage - its position is maintained by several ligaments a. splenophrenic b. splenorenal c. splenocolic d. gastrosplenic – short gastric a.

E N D
I. Anatomy - weight – approximately 100-150 grams - located in the left upper and protected by the lower portion of the rib cage - its position is maintained by several ligaments a. splenophrenic b. splenorenal c. splenocolic d. gastrosplenic – short gastric a.
- it is supplied by the splenic artery, which is a branch of the coeliac artery. - accessory spleens have been reported in 14% to 30%, ususally seen at the hilum, greater omentum, and ligaments of the spleen
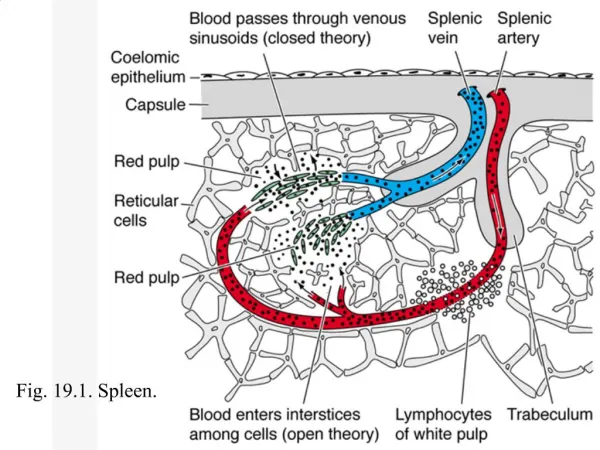
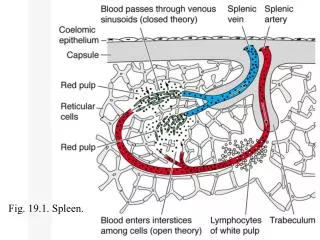
- consists of the capsule and trabeculae which enclose the pulp. - 3 zones of the pulp a. White pulp – lymph node; contains lymphocytes, macrophages, and plasma cells in a reticular network b. Red pulp – consists of the cord and sinuses; contains the cellular elements of the blood c. Marginal zone – poorly defined vascular space between pulps; contains sequestered foreign material and plasma as well as abnormal cellular elements
II. Physiologic Functions A. Filtering – splenic blood flow – 350 ml/day 1. removal of abnormal red blood cells – approximately 20 ml of aged RBC are removed daily 2.removal of abnormal WBC, plateletes
B. Immunologic Function 1. opsonin production 2. antibody synthesis (IgM) 3. protection from infection C. Storage Function 1. plateletes – 1/3 are stored in the spleen 2. in splenomegaly, up to 80% of the plateletes may be stored in the spleen thrombocytopenia
III. Diagnostic A. Evaluation of size 1. physical examination a. not normally palpable b. felt in 2% of healthy adults c. no significant dullness elicited by percussion over spleen d. as organ enlarges, dullness is detected at the level of the 9th ICS in the left anterior axillary line
2. CT/MRI – depicts the spleen and defines abnormalities in size, shape and parenchymal pathology 3. 99 Tc colloid B. Evaluation of function 1. hypersplenism – reduction in number of RBC, WBC, plateletes 2. increase in cellular destruction results in compensatory rise in production in the bone marrow reticulocytosis
IV. Pathologies A. Rupture of the Spleen 1. Etiology – disruption of the spleen’s parenchyma, capsule, and blood supply a. spleen is the most commonly injured organ following blunt trauma b. 2% splenic injury during surgery in the LUQ – Gastric surgery c. spontneous rupture – hematologic disorders
2. Pathology a. splenic rupture i. intraperitoneal bleed ii. 90% of blunt trauma b. delayed rupture i. interval of days or weeks between injury and bleeding; 10%-15%
ii. Quiescent period (of Baudette) persists for less than 7 days up to 2 weeks iii. related to temporary tamponade of minor lacerations or slowly enlarging subcapsular hematoma
c. occult splenic rupture - pseudocyst of the spleen (1%) 3. Clinical manifestation a. hypovolemia/tchycardia b. hypotension c. localized (LUQ) or generalized abdominal pain d. Kehr’s sign – pain at the tip of the left shoulder diaphragmatic irritation e. Balance’s sign ( mass or fixed dullness at the left upper quadrant
4. diagnostic studies a. CBC – serial Hct determination leukocytosis b. x-ray of the abdomen i. fractured ribs ii. elevated immobile diaphragm iii. enlarged splenic shadow iv. medial displacement of gastric shadow v. widening shadow between splenic flexure and preperitoneal fat
c. CT scan d. angiography 5. Treatment – surgery a. children – delayed surgical management b. adult - splenectomy c. splenectomized patients should receive pneumovax Haemophilus influenza vaccine and children should also be given oral penicillin daily until age 18
B. Hypersplenism 1. Primary hyperslenism a. diagnosis by exclusion made after secondary hypersplenism has been excluded b. rare entity affecting women c. anyone or all formed elements may be affected d. enlarged spleen e. recurring fever and infection f. lymphoma and leukemia g. responds to splenectomy h. steroids do not improve condition
2. Secondary hypersplenism – caused by an identifiable underlying disease a. portal hypertension i. splenic congestion ii. most common cause of secondary hypersplenism iii. does not warrant splenectomy
b. splenic vein thrombosis i. massive splenomegaly ii. thrombosis secondary to pancreatitis iii. associated with bleeding esophageal varices iv. cured by splenectomy
c. other causes i. neoplasms – leukemia, lymphoma, metastatic carcinoma ii. myelproliferative disorders iii. increase in RBC destruction – thalassemia major iv. disorders in immune response – infectious mononucleosis, Felty’s syndrome (rheumatoid arthritis, splenomegally, neutropenia) v. diseases that infiltrate the spleen – amyloidosis, sarcoidosis
V. Splenectomy A. Absolute Indications for Splenectomy 1. splenic tumors – echinoccocal cyst 2. metastatic disease 3. splenic abscess 4.hereditary spherocytosis – most common hemolytic anemia for which splenectomy is indicated 5. bleeding esophageal varices
6. chronic lymphocytic leukemia 7. hairy cell leukemia 8. Chronic myeloid leukemia – more to ease the pain 9. Sarcomas 10 trauma
B. Relative indications for splenectomy 1. congenital hemolytic anemias 2. sickle cell anemia 3. idiopathic autoimmune hemolytic anemia 4. Thrombocytic thrombocytopenic purpura
5. Felty’s syndrome/Sarcoidosis (non-caseating granulomas)/Gaucher’s disease (lipid storage disease)/Niemann-Pick disease (abnormal storage of cholesterol and sphingomyelin)/Amyloidosis (abnormal extracellular storage of protein) 6. Chronic rheumatoid arthritis 7. granulocytopenia 8. Hodgkin’s lymphoma 9. Non-hodgekin’s lymphoma 10. idiopathic thrombocytopenic purpura
VI. Splenectomy Outcomes - post-operative appearance of: a. siderocytes b. Howell-Jolly bodies c. leukocytosis d. increased platelete count
A. Complications 1. left lower lobe atelectasis – most common 2. subphrenic hematoma 3. subphrenic abscess – can occur with placement of a drain 4. pancreatitis – trauma to the tail of the pancreas 5. deep vein thrombosis – low dose anticoagulants
B. Hematologic outcomes 1. initial a. thrombocytopenia – rise in platelete count within a few days b. chronic hemolytic anemias – Hgb level above 10 g/dl
2. long-term a. increase in platelete count– rise to >150,000 more than 2 months after surgery b. 90-100% success for hereditary spherocytosis
C. Overwhelming Post-Splenectomy Infection (OPSI) 1. lifetime risk of severe infection 2. incidence of 3.2% post-splenectomy 3. loss of the spleen’s ability to filter and phagocytose bacteria and infected RBC
4. most common sources of infection a. Streptococcus pneumoniae – most common b. Heamophilus influenzae B c. meninggococcus d. group A streptococci 5. presents with pneumonia or meningitis
6. risk factors for the development of OPSI a. indication for splenectomy - hematologic disorder vs trauma b. overall immune status c. interval from the date of surgery – usually within 2 years
7. prevention a.vaccine against i. pneumoccocus ii. H. influenzae iii. meninggococcus - to be given within 7-14 days after splenectomy
b. booster dose for pneumococcal vaccine every 5-6 years c. annual influenza vaccine d. daily dose of penicillin or amoxycillin for 2 years