Download
1 / 37
370 likes | 465 Views
The Story of the Toronto Central Local Integrated Network 2010 G20 Dashboard. Why we should look at it Again Laurie Mazurik MD FRCPC MBA Project Lead, Pandemic Orange. Special Acknowledgement. In 2010 TCLHIN went to extraordinary lengths to support their

E N D
The Story of the Toronto Central Local Integrated Network2010 G20 Dashboard Why we should look at it Again Laurie Mazurik MD FRCPC MBA Project Lead, Pandemic Orange
Special Acknowledgement In 2010 TCLHIN went to extraordinary lengths to support their Stakeholders as they prepared for very real threats to their ability to deliver patient care during the 2010 G20 Summit. The journey was a fascinating exploration of relationships and innovative thinking. All those involved applaud their initiative and leadership. http://www.torontocentrallhin.on.ca/
Laurie Mazurik MD (The Story Teller) Specialist in Emergency Medicine, Sunnybrook Hospital, Toronto Critical Care Transport Physician (Air and Land) Strategic Lead, Disaster and Emergency Preparedness Sunnybrook Member of Ontario SARS Operation Centre 2003 Conducted over 40 mass casualty health care system simulations since 2003 TCLHIN Lead for 2010 G20 Summit Preparations
There is lots of money to prepare 1 billion dollars for security (prevention) ~Almost 0$ for health care. It’s a good “learning” opportunity
We learned • What a HIRA is. Do you know? • That Security/Police thought the best place to hold protest marches is as close to 6 major Toronto hospitals as possible (They were the usual Protest Areas) • How to CUUS and SBAR • That Information is the new gold
Lots of hints about concerns International Politics Lingering Worry http://goo.gl/xTsLvP
We Did become Worried Overcrowded ED’s
Let’s Think SMART We just need Information IMS…no so effective We are not like police or military who use a hierarchal system daily We think triage, capacity and patient flow We can live with “liaison” and “in-charge”
Speak in SBAR,CUUS and Capacity Consistent and Easy to Use 13
SBAR: Acronym • S=situation: Briefly describe the current situation. • B=background: State the pertinent history. • A=assessment: Summarize the facts and what you think the problem is • R=recommendation: What you think needs to be done in order to be address the problem safely and effectively
Situation In critical events it is very difficult to get timely,credible information It is disparate Incomplete
Background There 3 main sources of information Media = fast not always credible EMS =relatively fast, credible, does not include ambulatory surge Phone who you know= piece meal, usually they don’t know either
Assessment If a critical incident occurs we will have a delayed indecisive and response Will not be able to provide EMS with credible information to justify diversion of selected ambulances away from hospitals
Recommendation Capture and Share Credible information in real-time Work with EMS to distribute surges across ALL health care resources Preserve Acute Care CRITICAL Services that other hospitals do not have
Talk about Capacity and set thresholds for Alerts • N= normal capacity =Green • 10-20% over N= Yellow • >20% = Red • Overwhelmed • Unable to Provide Service
Critical Language used:CUUS • Key Phrases must be understood by ALL to mean “STOP and Listen”-we have a potential problem • Example: United Airlines “CUUS” Program I am Concerned I am Uncomfortable This is Unsafe I am Scared
TC LHIN Background Submit Situational Report
Triggers Telco between TCLHIN Leads,Hospital Leads, TEMS, CritiCall,ORNGE & MOH TC LHIN Background Submit Situational Report
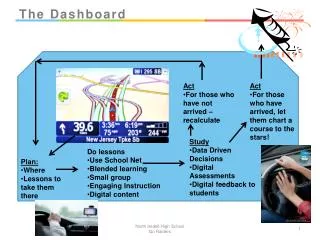
We Build “Smart System” • Based it on Media Display Systems • Used Terminology we could understand • Defined the Data we wanted in real-time • The way in which we wanted it reported and displayed • Set thresholds for Alerts or Alarms • Approached the TCLHIN to help us
How did it perform? • Hospital security provided info faster than media or police • Coordinated diversion of ambulances to “open” hospitals • Everyone understood the plan
Now We want to Build a New Prototype with End-user Input Giving Health Care Providers a chance to capture data and exchange ideas across a greater network
Value • Track trends • Look at Consequences • Identify Predictable Patterns • Build Strategies to Mitigate • Examine what others do in a broader network • Build/Test Models
Join The CBRNE Collaborative Time Limited Offer Explore the actual G20 Dashboard and give us feedback Do the polls in our e-learning modules and join some discussions Share your ideas and lets grow them together.