Download
1 / 19
190 likes | 324 Views
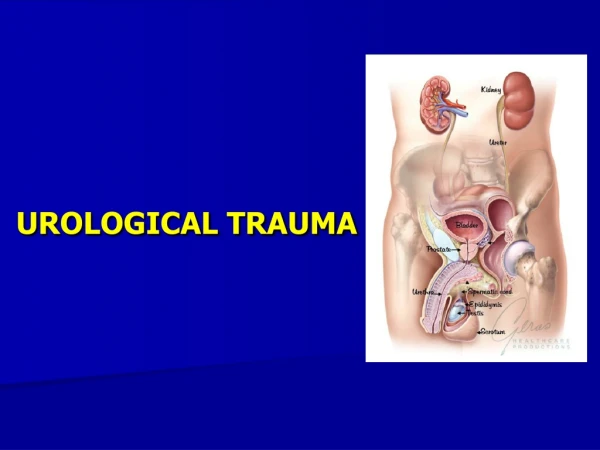
ADVANCED UROLOGICAL CASES DONE LAPAROSCOPICALLY. Dr. Anmar Nassir, FRCS(C) Fellowship in Andrology (U of Ottawa) Fellowship in EndoUrology and Laparoscopy (McMaster Univ) Chairman, Department of Surgery Umm Al-Qura Univ Consultant Urology, King Faisal Specialist Hospital, Jeddah.

E N D
Dr. Anmar Nassir, FRCS(C) Fellowship in Andrology (U of Ottawa) Fellowship in EndoUrology and Laparoscopy (McMaster Univ) Chairman, Department of Surgery Umm Al-Qura Univ Consultant Urology, King Faisal Specialist Hospital, Jeddah
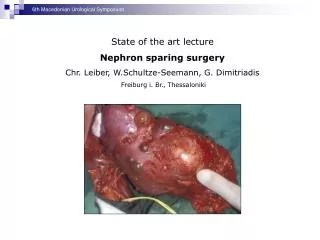
Advanced renal laparoscopy In-situ intracorporeal renal hypothermia is obtained with a Pruit balloon catheter (insert), End-to end splenorenal anastomosis made using needlescopic instruments SIDNEY, GILL. BJU international 2005
Advanced renal laparoscopy Laparoscopic renal autotransplantation End-to-side anastomosis of the renal artery and vein to the common iliac artery and vein Created using free-hand laparoscopic techniques SIDNEY, GILL. BJU international 2005
Advanced renal laparoscopy SIDNEY, GILL. BJU international 2005
Advanced renal laparoscopy SIDNEY, GILL. BJU international 2005
Hand-port incisional hernias • 50 laparoscopic hand-assisted radical nephrectomies. • Closed with #1 polydioxanone sulfate suture in a running fashion. • Three (6%) patients developed All in midline hand-port sites. • The average body weight of those who developed an incisional hernia was 137 kg. JSLS, 9: 196–198, 2005
Hand-port incisional hernias • Risk Factors • obesity • earlier return to activity of • Conclusion: • nonabsorbable suture + interrupted closure • limited activity 4-6 wks post op if high risks. • No further wound hernias since adopting these changes JSLS, 9: 196–198, 2005 Clayman. J of Urol, Dec 2005
WOUND COMPLICATIONS AFTER HALS MONTGOMERY, et al. J of Uro, Dec 2005
WOUND COMPLICATIONS AFTER HALS MONTGOMERY, et al. J of Uro, Dec 2005
HAL Adrenalectomy • The spleen is fully mobilized cephalad so that it falls medially and does not need retraction. • The dissection is carried posteriorly to the tail of the pancreas, which is rotated medially as well. • The table is further tilted in reverse-Trendelenburg position to allow caudal displacement of surrounding organs. • The dissection of the gland starts inferiomedially, controlling the left adrenal vein initially, if possible. • The lateral attachments to the adrenal gland are taken down with either the monopolar hook or the ultrasonic coagulating shears (Ethicon, Cincinnati, Ohio). Cobb et al. April 2005, American Journal of Surgery
Hand-assisted laparoscopy provides a nice alternative to the open technique for large adrenal tumors and obese patients. • facilitate dissection, retraction, and removal of an intact gland. • A fourth trocar is necessary on the right to retract the liver and expose the most medial aspect of the adrenal gland and inferior vena cava Cobb et al. April 2005, American Journal of Surgery
laparoscopic Palomo varicocelectomy Kole, J Urol. 2004;172:1749 • 6% incidence of post op hydrocele formation in 98 pts • Lymphatic sparing laparoscopic surgery. To do so they placed the laparoscopic lens close to the surgical field, (20×) thus, decreasing the development of hydrocele to 2 %. • 2 ml methylene blue is injected into the space between the tunica vaginalis and tunica albuginea. During diagnostic laparoscopy, the blue-stained lymphatic trunks can be easily separated from the testicular vess. Kocvara et al, J Urol, 173: 1751, 2005 Ben-Meir et al, J Urol. December 2005
Complications Anticipate & prevent Take care of the details Recognize & manage CONVERSION should not be a sign of shame ( Vallencian, et.al. J. Urol,2002)
Ergonomics • 8-22 of Lap. Surgeons reported pain, numbness, stiffness and eye strain (Hemal, 2002) • It is due to; • Posture • Visualization • Manipulation • Monitor should be at the head level or 10-20 degrees lower • Use step stool to work comfortably
Future • Better equipment & agents • Simulators • Robotics • Telesurgery
OR1 WebSurg 1 place de l'Hôpital, BP 426 F-67091 Strasbourg cedex, FRANCE http://www.websurg.com