Download
1 / 5
50 likes | 192 Views
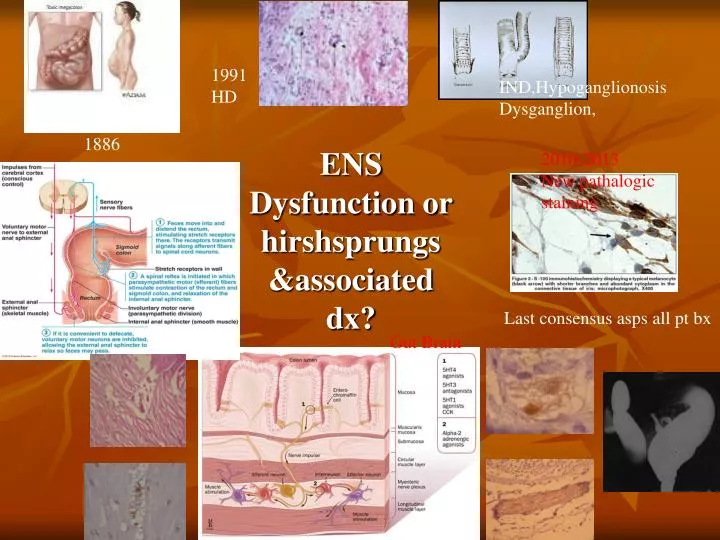
1991 HD. IND,Hypoganglionosis Dysganglion,. 1886. ENS Dysfunction or hirshsprungs &associated dx?. 2010-2013 New pathalogic staining. Last consensus asps all pt bx. Gut Brain.

E N D
1991 HD IND,Hypoganglionosis Dysganglion, 1886 ENS Dysfunction or hirshsprungs &associated dx? 2010-2013 New pathalogic staining Last consensus asps all pt bx Gut Brain
Method:From January 2010 to February 2012 , In 40 children with chronic constipation a control before and after clinical trial in two parallel groups study was performed .Rectal biopsy was done for pathologic evaluations. Immunostaining was performed for ganglion cells and also nerve fibers in different layers of bowel were evaluated in stained slides for Calretinin,C-kit,NSE as marker for ganglionecells,Cajal cells and nerve trunks
icc th All patient 1- adquate rx2- neonatal hx 3-distension 4-obstruction 5- kinds of incontinence 16 17 G+calret 18 G-calret N=31 No ganglione ENS dysfunctiion N=9 Full rectal bx Maturation icc Relaxing agent Nerve growth factor Blocking agents Dopamine inhibitor Increase acetylcholine Vesicule secretion 6-12 months Good ES tone
Results: In this study 9 aganglionic patients with mean age of 3.6 ± 1.7 years compared with 31hypoganglionic patients with mean age of 3.2 ± 1.2 years. Pultrough operation were done for all patients in anglionic group. But in hypoganglionic group Pultrough operation were done in six(19.4%) patients. postop manometry significantly was better in both groups, but monomeric • change wasn’t significant between two groups. 1-Rectum is gut brain,(even change proximal gut pathalogy[ped surg 2013]),pathalogic evaluation should be compelet(calret ,ache,h&e,c-kit,nse) 2-All chronic case need bx ,if treatment targeted ,there is a better results 3-The last Resort is to remove gut brain chemically or surgically to let the reminder work spontanousely however rx should be based clinically not on bx(ped surg 2013)
References 1- Foroutan HR, Hosseini SM, Banani SA, Bahador A, Sabet B, Zeraatian S, et al. Comparison of botulinium toxin injection and posterior anorectal myectomy in treatment of internal anal sphincter achalasia. Indian J Gastroenterol 2008;27:62-5. 2- Hosseini SM, Zarenezhad M, Hedjazi A, Khazdooz M, Falahi S. Treatment of constipation in children based on anorectal manometery findings. Ann Nigerian Med. 2012;6:22-5. 3- Hiradfar M, Sharifi N, Khajedaluee M, Zabolinejad N, Taraz Jamshidi S. Calretinin Immunohistochemistery: an aid in the diagnosis of Hirschsprung’s Disease. Iran J Basic Med Sci. 2012;15:1053-9. 4- Kustermann A, Neuhuber W, Brehmer A. Calretinin and somatostatin immunoreactivities label different human submucosal neuron populations. Anat Rec (Hoboken). 2011;294:858-69. 5- Kubota M, Suita S, Kamimura T, Ito Y, Szurszewski JH. Electrophysiological properties of the aganglionic segment in Hirschsprung's disease. Surgery. 2002;131(1 Suppl):S288-93. 6- Kapur RP, Reed RC, Finn LS, Patterson K, Johanson J, Rutledge JC. Calretinin immunohistochemistry versus acetylcholinesterase histochemistry in the evaluation of suction rectal biopsies for Hirschsprung Disease. Pediatr Dev Pathol. 2009;12:6-15. 7- Guinard-Samuel V, Bonnard A, De Lagausie P, Philippe-Chomette P, Alberti C, El Ghoneimi A, et al. Calretinin immunohistochemistry: a simple and efficient tool to diagnose Hirschsprung disease. Mod Pathol. 2009;22:1379-84. 8- Hosseini SM, Foroutan HR, Bahador A, Khosravi MB, Geramizadeh B, Sabet B, et al. Role of rectal biopsy in predicting response to intrasphincteric botulinum toxin injection for obstructive symptoms after a pullthrough operation. Indian J Gastroenterol 2008;27:99-102.