Download
1 / 46
1.05k likes | 2.94k Views
INFECTIVE ENDOCARDITIS. Vegetations (arrows) due to viridans streptococcal endocarditis involving the mitral valve. Infective endocarditis (IE) is an infection of the endocardial surface of the heart.

E N D
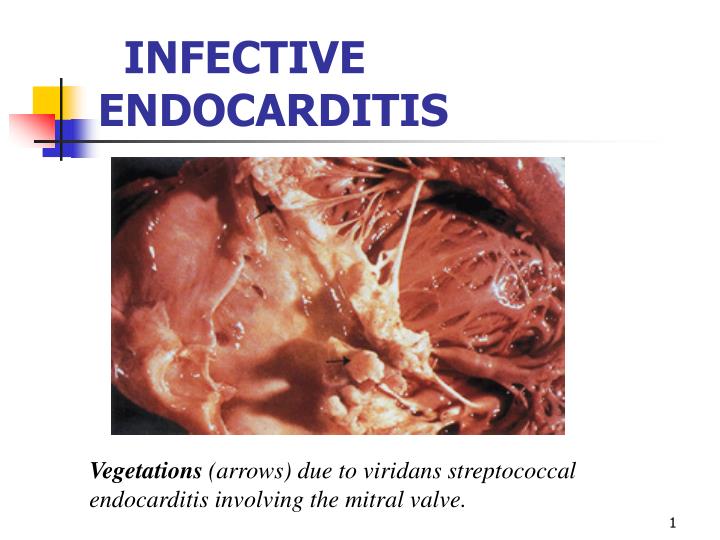
INFECTIVE ENDOCARDITIS Vegetations (arrows) due to viridans streptococcal endocarditis involving the mitral valve.
Infective endocarditis (IE) is an infection of the endocardial surface of the heart. • The intracardiac effects of this infection include severe valvular insufficiency, which may lead to congestive heart failure and myocardial abscesses. IE also produces a wide variety of systemic signs and symptoms through several mechanisms, including both sterile and infected emboli and various immunological phenomena.
ETIOLOGYOrganisms Causing Major Clinical Forms of Endocarditis: • Staphylococcus aureusinfection is the most common cause of IE, including PVE, acute IE, and IVDA IE. • Approximately 35-60.5% of staphylococcal bacteremias are complicated by IE. • More than half the cases are not associated with underlying valvular disease. • The mortality rate of S aureus IE is 40-50%.
ETIOLOGYOrganisms Causing Major Clinical Forms of Endocarditis: • Streptococcus viridans • This organism accounts for approximately 50-60% of cases of subacute disease. • Most clinical signs and symptoms are mediated immunologically. • Streptococcus intermedius group • These infections may be acute or subacute. • S intermedius infection accounts for 15% of streptococcal IE cases. • S intermedius is unique among the streptococci; it can actively invade tissue and can cause abscesses.
ETIOLOGYOrganisms Causing Major Clinical Forms of Endocarditis: • Nonenterococcal group D organisms • The clinical course is subacute. • Infection often reflects underlying abnormalities of the large bowel (eg, ulcerative colitis, polyps, cancer). • The organisms are sensitive to penicillin. • Group B streptococci • Acute disease develops in pregnant patients and older patients with underlying diseases (eg, cancer, diabetes, alcoholism). • The mortality rate is 40%. • Complications include metastatic infection, arterial thrombi, and congestive heart failure. • It often requires valve replacement for cure. • Group A, C, and G streptococci • Acute disease resembles that of S aureus IE (30-70% mortality rate), with suppurative complications. • Group A organisms respond to penicillin alone. • Group C and G organisms require a combination of synergistic antibiotics (as with enterococci).
ETIOLOGYOrganisms Causing Major Clinical Forms of Endocarditis: • Coagulase-negative S aureus • This causes subacute disease. • It behaves similarly to S viridans infection. • It accounts for approximately 30% of PVE cases and less than 5% of NVE cases.10 • Pseudomonas aeruginosa • This is usually acute, except when it involves the right side of the heart in IVDA IE. • Surgery is commonly required for cure. • HACEK organisms (ie, Haemophilus aphrophilus, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, Kingella kingae) • These organisms usually cause subacute disease. • They account for approximately 5% of IE cases. • They are the most common gram-negative organisms isolated from patients with IE. • Complications may include massive arterial emboli and congestive heart failure. • Cure requires ampicillin, gentamicin, and surgery.
ETIOLOGYOrganisms Causing Major Clinical Forms of Endocarditis: • Fungi • These usually cause subacute disease. • The most common organism of both fungal NVE and fungal PVE is Candida albicans. • Fungal IVDA IE is usually caused by Candida parapsilosis or Candida tropicalis. • Aspergillus species are observed in fungal PVE and NIE.
Acute endocarditis usually occurs when heart valves are colonized by virulent bacteria in the course of microbemia. The most common cause of acute endocarditis is Staphylococcus aureus; other less common causes are Streptococcus pneumoniae, Neisseria gonorrhoeae, Streptococcus pyogenes, and Enterococcus faecalis.
Patients with subacute endocarditis usually have underlying valvular heart disease and are infected by less virulent organisms such as viridans streptococci, enterococci, nonenterococcal group D streptococci, microaerophilic streptococci, and Haemophilus species.
Bacteremia can result from various invasive procedures • Endoscopy • Rate of 0-20% • CoNS, streptococci, diphtheroids • Colonoscopy • Rate of 0-20% • Escherichia coli, Bacteroides species • Barium enema • Rate of 0-20% • Enterococci, aerobic and anaerobic gram-negative rods • Dental extractions • Rate of 40-100% • S viridans • Transurethral resection of the prostate • Rate of 20-40% • Coliforms, enterococci, S aureus • Transesophageal echocardiography • Rate of 0-20% • S viridans, anaerobic organisms, streptococci
PATHOPHYSIOLOGYThe clinical manifestations of IE result from: • 1. Local destructive effects of intracardiac infection (distortionor perforation of valve leaflets, rupture of chordaetendineae, perforations or fistulas between major vessels and cardiac chambers, functional valvular stenosis) with congestive heart failure; • 2. Embolization of fragments of the vegetation, resulting in infection or infarction including the spleen, kidney, meninges, brain, bone, pericardium, synovium; • 3. The hematogenous seeding of remote sites during continuous bacteremia (hyper-gammaglobulinemia, cryoglobulins, splenomegaly); • 4. Immunologic response to the infection with tissue injury due to deposition of preformed immune complexes or antibody-complement interaction with antigens deposited in tissues (glomerulonephritis, Osler’s nodes, rheumatological manifestations).
Clinical and Laboratory Features of Infective Endocarditis • Fever80-90 % • Chills and sweats40-75 % • Anorexia, weight loss, malaise25-50 % • Myalgias, arthralgias15-30 % • Back pain7-15 % • Heart murmur80-85 % • New/worsened regurgitant murmur10-40 %
Clinical and Laboratory Features of Infective Endocarditis • Arterial emboli20-50 % • Splenomegaly15-50 % • Clubbing10-20 % • Neurologic manifestations20-40 % • Peripheral manifestations (Osler's nodes, subungual hemorrhages, Janeway lesions, Roth's spots) 2-15 %
Clinical and Laboratory Features of Infective Endocarditis • Petechiae 10-40 % • Laboratory manifestations: • Anemia70-90 % • Leukocytosis20-30 % • Microscopic hematuria30-50 % • Elevated erythrocyte sedimentation rate>90 %
Clinical and Laboratory Features of Infective Endocarditis • Rheumatoid factor50 % • Circulating immune complexes65-100 % • Decreased serum complement5-40 %
Common Peripheral Manifestations of Infective Endocarditis.Splinter hemorrhages (A) are normally seen under the fingernails. They are usually linear and red for the first-two to three days and brownish thereafter.Panel B shows conjunctival petechiae.Osler's nodes (Panel C) are tender, subcutaneous nodules, often in the pulp of the digits or the thenar eminence.Janeway's lesions (Panel D) are nontender, erythematous, hemorrhagic, or pustular lesions, often on the palms or soles.
Noncardiac Manifestations Janeway’s lesions. Hemorrhagic, infarcted macules and papules on the volar fingers in a patient with S. aureus endocarditis.
Noncardiac Manifestations Septic vasculitis associated with bacteremia. Dermal nodule with hemorrhage and necrosis on the dorsum of a finger. This type of lesion occurs with bacteremia (e.g., S. aureus) and fungemia (e.g., Candida tropicalis).
Noncardiac Manifestations subconjunctival hemorrhage. Submucosal hemorrhage of the lower eyelid in an elderly diabetic with enterococcal endocarditis; splinter hemorrhages in the midportion of the nail bed and Janeway lesions were also present.
Noncardiac Manifestations Splinter hemorrhages, embolic Subungual hemorrhages in the midportion of the nail bed (quite different in comparison to traumatic splinter hemorrhages) was noted in several fingernails in a 60-year-old female with enterococcal endocarditis, who had associated subconjunctival hemorrhage.
Splinter haemorrhages are linear haemorrhages lying parallel to the long axis of finger or toe nails.
Noncardiac Manifestations Osler's nodes. Violaceous, tender nodules on the volar fingers associated with minute infective emboli or immune complex deposition.
Noncardiac Manifestations Septic emboli with hemorrhage and infarction due to acute Staphylococcus aureus endocarditis.
Noncardiac Manifestations Vasculitis
Clubbing. Seen in patients with chronic lung disease, cyanotic heart disease, cirrhosis and infective endocarditis.
Infective endocarditis: metastatic infections due to emboli.
Noncardiac Manifestations Computed tomography of the abdomen showing large embolic infarcts in the spleen and left kidney of a patient with Bartonella endocarditis.
The Duke Criteria for the Clinical Diagnosis of Infective Endocarditis • Positive blood culture for Infective EndocarditisTypical microorganism consistent with IE from 2 separate blood cultures, as noted below:• viridans streptococci, Streptococcus bovis, or HACEK group, or • • community-acquired Staphylococcus aureus or enterococci, in the absence of a primary focus • or • Microorganisms consistent with IE from persistently positive blood cultures defined as:• 2 positive cultures of blood samples drawn >12 hours apart, or • • all of 3 or a majority of 4 separate cultures of blood (with first and last sample drawn 1 hour apart)
The Duke Criteria for the Clinical Diagnosis of Infective Endocarditis • MAJOR CRITERIA: • Evidence of endocardial involvement • Positive echocardiogram - Oscillating intracardiac mass on valve or supporting structures or in the path of regurgitant jets or in implanted material, in the absence of an alternative anatomic explanation, or - Abscess, or - New partial dehiscence of prosthetic valve, or • New valvular regurgitation (increase or change in preexisting murmur not sufficient)
The Duke Criteria for the Clinical Diagnosis of Infective Endocarditis • MINOR CRITERIA: • Predisposition: predisposing heart condition or injection drug use • Fever ≥38.0◦C • Vascular phenomena: major arterial emboli, septic pulmonary infarcts, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, Janeway lesions • Immunologic phenomena: glomerulonephritis, Osler's nodes, Roth's spots, rheumatoid factor
The Duke Criteria for the Clinical Diagnosis of Infective Endocarditis • MINOR CRITERIA: • Microbiologic evidence: positive blood culture but not meeting major criterion as noted previously or serologic evidence of active infection with organism consistent with infective endocarditis • Echocardiogram: consistent with infective endocarditis but not meeting major criterion
The Duke Criteria for the Clinical Diagnosis of Infective Endocarditis • Documentation of two major criteria, of one major and three minor criteria, or of five minor criteria allows a clinical diagnosis of definite endocarditis.
INFECTIVE ENDOCARDITIS Vegetations (arrows) due to viridans streptococcal endocarditis involving the mitral valve.
Characteristic sites of vegetations within the heart. In the presence of aortic insufficiency, vegetations characteristically occur on the ventricular surface of the aortic valve (A) or on the chordae tendinae or papillary muscles (B). In mitral regurgitation, the vegetations characteristically are located on the atrial surface of the mitral valve (C) or at sites of jet lesions (D) on the atrial wall.
Acute Affects normal heart valves Rapidly destructive Metastatic foci Commonly Staph. If not treated, usually fatal within 6 weeks Subacute Often affects damaged heart valves Indolent nature If not treated, usually fatal by one year Further Classification
Antibiotic Treatment for Infective Endocarditis Caused by Common Organisms • StreptococciPenicillin-susceptible streptococci, S. bovis • Penicillin G 2-3 million units IV q4h for 4 weeks • Penicillin G 2-3 million units IV q4h plus gentamicin 1 mg/kg IM or IV q8h, both for 2 weeks • Ceftriaxone 2 g/d IV as single dose for 4 weeks • Vancomycind 15 mg/kg IV q12h for 4 weeks
Antibiotic Treatment for Infective Endocarditis Caused by Common Organisms • Relatively penicillin-resistant streptococci - Penicillin G 3 million units IV q4h for 4-6 weeks plus gentamicin 1 mg/kg IV q8h for 2 weeks • Penicillin-resistant streptococci, pyridoxal-requiring streptococci (Abiotrophia spp.) - Penicillin G 3-4 million units IV q4h plus gentamicinc 1 mg/kg IV q8h, both for 4-6 weeks
Indications for Cardiac Surgical Intervention in Patients with Endocarditis • Surgery required for optimal outcome • Moderate to severe congestive heart failure due to valve dysfunction • Partially dehisced unstable prosthetic valve • Persistent bacteremia despite optimal antimicrobial therapy • Lack of effective microbicidal therapy (e.g., fungal or Brucella endocarditis) • S. aureus prosthetic valve endocarditis with an intracardiac complication • Relapse of prosthetic valve endocarditis after optimal antimicrobial therapy • Persistent unexplained fever (≥10 days) in culture-negative prosthetic valve endocarditis
Indications for Cardiac Surgical Intervention in Patients with Endocarditis • Surgery to be strongly considered for improved outcomea • Perivalvular extension of infection • Poorly responsive S. aureus endocarditis involving the aortic or mitral valve • Large (>10-mm diameter) hypermobile vegetations with increased risk of embolism • Persistent unexplained fever (≥10 days) in culture-negative native valve endocarditis • Poorly responsive or relapsed endocarditis due to highly antibiotic-resistant enterococci or gram-negative bacilli
Prevention • Approximately 15-25% of cases of IE are a consequence of invasive procedures that produce a significant bacteremia. Because only 50% of those who developed valvular infection following a procedure were identified as being candidates for antibiotic prophylaxis, only approximately 10% of cases of IE can be prevented by the administration of preprocedure antibiotics. • Maintaining good oral hygiene is probably more effective in the overall prevention of valvular infection because gingivitis is the most common source of spontaneous bacteremias. • The American Heart Association periodically compiles recommendations for IE prophylaxis.