Download
1 / 1
10 likes | 181 Views
Susceptibility of Drug Resistant Acinetobacter baumanii (DRAB) to a stabilized aqueous allicin extract from garlic (AB1000 ). Researchers’/Presenters’ Names Institution/Organization/Company.

E N D
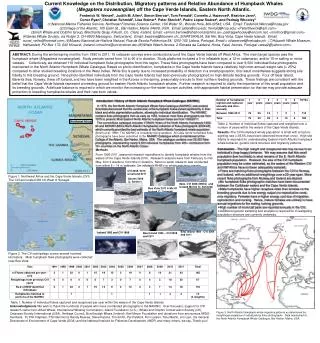
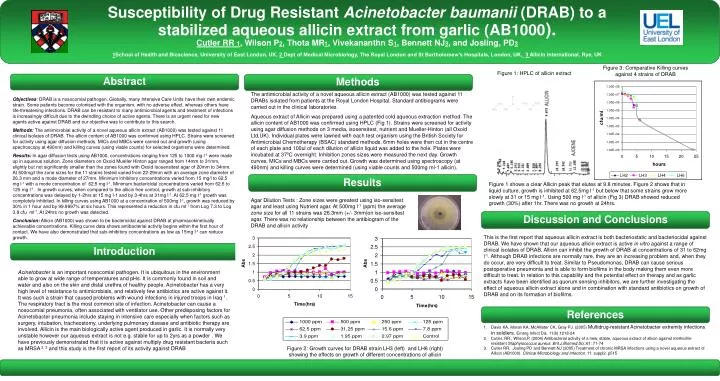
Susceptibility of Drug Resistant Acinetobacter baumanii (DRAB) to a stabilized aqueous allicin extract from garlic (AB1000). Researchers’/Presenters’ NamesInstitution/Organization/Company Susceptibility of Drug Resistant Acinetobacter baumanii (DRAB) to a stabilized aqueous allicin extract from garlic (AB1000).Cutler RR 1, Wilson P2, Thota MR1, Vivekananthn S1, Bennett NJ3, and Josling, PD31School of Health and Bioscience, University of East London, UK, 2 Dept of Medical Microbiology, The Royal London and St Bartholomew’s Hospitals, London, UK,3 Allicin International, Rye, UK Figure 3: Comparative Killing curves against 4 strains of DRAB Figure 1: HPLC of allicin extract Abstract Methods The antimicrobial activity of a novel aqueous allicin extract (AB1000) was tested against 11 DRABs isolated from patients at the Royal London Hospital. Standard antibiograms were carried out in the clinical laboratories. Aqueous extract of Allicin was prepared using a patented cold aqueous extraction method. The allicin content of AB1000 was confirmed using HPLC (Fig 1). Strains were screened for activity using agar diffusion methods on 3 media, isosensitest, nutrient and Mueller-Hinton (all Oxoid Ltd,UK). Individual plates were lawned with each test organism using the British Society for Antimicrobial Chemotherapy (BSAC) standard methods. 6mm holes were then cut in the centre of each plate and 100ul of each dilution of allicin liquid was added to the hole. Plates were incubated at 370C overnight. Inhibition zones sizes were measured the next day. Growth curves, MICs and MBCs were carried out. Growth was determined using spectroscopy (at 490nm) and killing curves were determined (using viable counts and 500mg ml-1 allicin). Objectives: DRAB is a nosocomial pathogen. Globally, many Intensive Care Units have their own endemic strain. Some patients become colonised with the organism, with no adverse effect, whereas others have life-threatening infections. DRAB can be resistant to many antimicrobial agents and treatment of infections is increasingly difficult due to the dwindling choice of active agents. There is an urgent need for new agents active against DRAB and our objective was to contribute to this search. Methods: The antimicrobial activity of a novel aqueous allicin extract (AB1000) was tested against 11 clinical isolates of DRAB. The allicin content of AB1000 was confirmed using HPLC. Strains were screened for activity using agar diffusion methods. MICs and MBCs were carried out and growth (using spectroscopy at 490nm) and killing curves (using viable counts) for selected organisms were determined. Results: In agar diffusion tests using AB1000, concentrations ranging from 125 to 1000 mg l-1 were made up in aqueous solution. Zone diameters on Oxoid Mueller Hinton agar ranged from 14mm to 31mm, slightly but not significantly smaller than the zones found with Oxoid Isosensitest agar of 20mm to 34mm. At 500mg/l the zone sizes for the 11 strains tested varied from 22-29mm with an average zone diameter of 26.3 mm and a mode diameter of 27mm. Minimum inhibitory concentrations varied from 15 mg/l to 62.5 mg l-1 with a mode concentration of 62.5 mg l-1. Minimum bactericidal concentrations varied from 62.5 to 125 mg l-1. In growth curves, when compared to the allicin free control, growth at sub-inhibitory concentrations was delayed by 1-2hrs at 15 mg l-1 and by 3-4hrs at 31mg l-1. At 62.5 mg l-1 growth was completely inhibited. In killing curves using AB1000 at a concentration of 500mg l-1, growth was reduced by 30% in 1 hour and by 99.9997% at six hours. This represented a reduction in cfu ml-1 from Log 7.3 to Log 3.8 cfu ml-1. At 24hrs no growth was detected. Conclusion: Allicin (AB1000) was shown to be bactericidal against DRAB at pharmacokinetically achievable concentrations. Killing curve data shows antibacterial activity begins within the first hour of contact. We have also demonstrated that sub-inhibitory concentrations as low as 15mg l-1 can reduce growth. (162) Results Figure 1 shows a clear Allicin peak that elutes at 9.8 minutes. Figure 2 shows that in liquid culture, growth is inhibited at 62.5mg l-1 but below that some strains grow more slowly at 31 or 15 mg l-1. Using 500 mg l-1 of allicin (Fig 3) DRAB showed reduced growth (30%) after 1hr. There was no growth at 24hrs. Agar Dilution Tests : Zone sizes were greatest using iso-sensitest agar and least using Nutrient agar. At 500mg l-1 (ppm) the average zone size for all 11 strains was 26.3mm (+/- 3mm)on iso-sensitest agar. There was no relationship between the antibiogram of the DRAB and allicin activity Discussion and Conclusions This is the first report that aqueous allicin extract is both bacteriostatic and bacteriocidal against DRAB. We have shown that our aqueous allicin extract is active in vitro against a range of clinical isolates of DRAB. Allicin can inhibit the growth of DRAB at concentrations of 31 to 62mg l-1. Although DRAB infections are normally rare, they are an increasing problem and, when they do occur, are very difficult to treat. Similar to Pseudomonas, DRAB can cause serious postoperative pneumonia and is able to form biofilms in the body making them even more difficult to treat. In relation to this capability and the potential effect on therapy and as garlic extracts have been identified as quorum sensing inhibitors, we are further investigating the effect of aqueous allicin extract alone and in combination with standard antibiotics on growth of DRAB and on its formation of biofilms. Introduction Acinetobacter is an important nosocomial pathogen. It is ubiquitous in the environment able to grow at wide range of temperatures and pHs. It is commonly found in soil and water and also on the skin and distal urethra of healthy people.Acinetobacter has a very high level of resistance to antimicrobials, and relatively few antibiotics are active against it. It was such a strain that caused problems with wound infections in injured troops in Iraq 1. The respiratory tract is the most common site of infection. Acinetobacter can cause a nosocomial pneumonia, often associated with ventilator use. Other predisposing factors for Acinetobacter pneumonia include staying in intensive care especially when factors such as surgery, intubation, tracheostomy, underlying pulmonary disease and antibiotic therapy are involved. Allicin is the main biologically active agent produced in garlic. It is normally very unstable however our aqueous extract is not e.g. stable for up to 2yrs as a powder . We have previously demonstrated that it is active against multiply drug resistant bacteria such as MRSA 2, 3 and this study is the first report of its activity against DRAB References • Davis KA, Moran KA, McAllister CK, Gray PJ. (2005) Multidrug-resistant Acinetobacter extremity infections in soldiers. Emerg Infect Dis. 11(8):1218-24 • Cutler, RR., Wilson,P. (2004) Antibacterial activity of a new, stable, aqueous extract of allicin against methicillin-resistant Staphylococcus aureus. Brit.J.Biomed.Sci.:61: 71-74 • Cutler RR, Josling PD and Bennett NJ (2005) Treatment of chronic MRSA infections using a novel aqueous extract of Allicin (AB1000). Clinical Microbiology and Infection. 11: suppl2. p515 Figure 2: Growth curves for DRAB strain LH3 (left) and LH6 (right) showing the effects on growth of different concentrations of allicin