Download
1 / 14
140 likes | 261 Views
Team Status Reports. Melbourne May 2010. “Hawke’s Bay District Health Board: Confidential document. This document is produced for the purposes of a ‘Protected Quality Assurance Activity’ under Health Practitioners’ (Quality Assurance Activity: Hawke’s Bay District Health Board) Notice 2005.”.

E N D
Team Status Reports Melbourne May 2010 “Hawke’s Bay District Health Board: Confidential document. This document is produced for the purposes of a ‘Protected Quality Assurance Activity’ under Health Practitioners’ (Quality Assurance Activity: Hawke’s Bay District Health Board) Notice 2005.”
Main Hospital Code Name: Fauna Current number of beds at main hospital : 350 Programme Team
Scope and boundaries of project Hawke’s Bay Hospital serving regional population of 155,000. Secondary level, approx 350 inpatient beds. Serving Chatham Islands and 2 small rural GP run satellite hospitals; Wairoa is 130km by road, patients transferred by air. Central Hawke’s Bay is 50km by road. Acute, Elective, Rehabilitation, Mental Health, Paediatric, Maternity Services. On site ICU, CCU, rehabilitation ward of 38 beds. HB hospital transfers out to Tertiary hospitals all patients requiring; Interventional Cardiology Neurosurgery Long stay project is focussing initially, on adult Medical and Surgical Services (all surgical specialties).
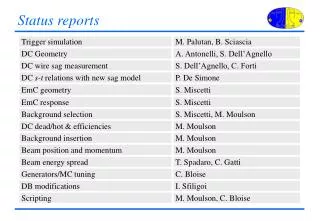
Long-stay Medical/Surgical/ Maternity Episodes 6 months data Fauna
Long-stay Medical/Surgical/ Maternity Bed Days 6 months data Fauna
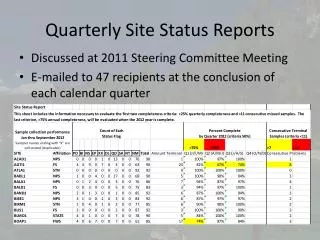
Data Table for Fauna NB. 20072008 6 months only
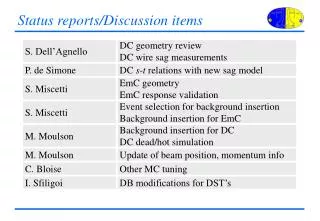
Data Issues • Transfer of acute patients to rehabilitation (and vice-versa) creates a new event due to rehabilitation contract requirements. • ICU patients are included in specialty data i.e. included in medical data if under medical team. This creates difficulties when trying to breakdown and analyse ICU patients
The Impact on the Patient- Case Study • 67 yo male admitted medical ward via ED, 6 days D&Vs, dehydrated • Acute renal failure –admission; bloods Creat 474, urea 33.6. BP75-85 • Seen by Physician on ward round = Thurs pre Easter. Fri & Mon rounds not done as public holidays. Next SMO review Day 8 (Thurs) • Taking multiple nephrotoxic drugs prescribed by GP, unknown to Medical team till after Physician round on day 2 • Severity & risks unrecognised, under treated/monitored for two days • Over treated on day 3 (5 litres IV), Kidneys recover but… • Develops gross oedema legs day 4 leading to blisters++ & skin breakdown starting on day 5, requires multiple skin dressings • Medication error – 400mg IV frusemide prescribed/given (not 40mg) • AF episodes through stay, stat medications, no long term Rx … • Social - discharge delayed as pt decides to convalesce in town 2 hours away
Issues and Observations about process to date • Good documentation of weekend plan by medical team • A lot of time required for reviewing patients • Clinicians suspicious around reasons for review of their patients • Difficulties factoring in rehabilitation patients moving in and out of acute services; • LOS/inpatient event reset with new episode of care every time patient transferred to/from acute services during same stay. • Inadequate documentation in patient notes; decision making, timing of interventions, request – action • Medical records poorly organised/ordered for this type of audit/review • Nursing documentation lacks variance reporting and documentation on some actions taken
Provisional Top 10 Diagnoses • Multiple medical teams → lack of clear responsibility • Senior Medical care inconsistent over long weekends • 3. Wound break down • 4. Inadequate documentation • 5. Discharge expectations of hospital discordant with patients & families expectations • 6. Inconsistent messages amongst MDT re discharge expectations • 7. Limited Allied Health cover in weekends and public holidays • 8. Weak discharge planning processes across MDT • 9. Long LOS for spinal patients requiring immobilisation • 10. Palliative Care inpatient services – community hospice closing