Download
1 / 49
490 likes | 591 Views
Speaker notes included in notes section below. Overview of the Obesity Epidemic. Obese (BMI ≥ 30) Overweight (BMI 25 - 29.9). More than 60% of US Adults Are Overweight or Obese.

E N D
Speaker notes included in notes section below Overview of the Obesity Epidemic
Obese (BMI ≥ 30) Overweight (BMI 25 - 29.9) More than 60% of US Adults Are Overweight or Obese Flegal K, et al. JAMA. 2002;288:1723-1727. Hedley AA, et al. JAMA. 2004;291:2847-2850.
Assessing Obesity: What Is BMI? • BMI • Calculated as weight(kg)/height(m2) • Evaluatesweight relative to height • Replaced % ideal body weight as the primary criterion for assessing obesity • Correlates significantly with body fat, morbidity, and mortality NIH Natl Heart, Lung, and Blood Inst. Obes Res. 1998;6(suppl 2):51S. Willett WC et al. N Engl J Med. 1999;341:427.
Obesity Trends by Gender and Ethnicity Men Women Flegal K, et al. JAMA 2002;288:1723-1727.
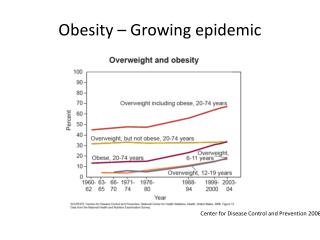
Prevalence of Overweight in Children and Adolescents Flegal K, et al. JAMA 2002;288:1723-1727. Hedley AA, et al. JAMA 2004;291:2847-2850.
BMI BMI BMI BMI For Children, BMI Changes with Age Boys: 2 to 20 years Example: 95th Percentile Tracking Age BMI 2 yrs 19.3 4 yrs 17.8 9 yrs 21.0 13 yrs 25.1
Fat stores Obesity is Caused by Long-Term Positive Energy Balance Energy expenditure Energy intake
BMI Obesity Predisposition Obesity Genetics vs Environment “Obesigenic”environment Restrictiveenvironment Resistant Prone Ravussin E, Bouchard C. Eur J Pharmacol. 2000;410:131-145.
Responding to the Obesity Epidemic • Create a child-healthy environment • Banish junk food from schools • Reduce food ads directed at children • Increase opportunities for physical activity
16 oz 32 oz 44 oz 52 oz 64 oz 1 oz ≈ 12 calories
% of Children with Daily Physical Education American Academy of Pediatrics.
40 NHES 1967-1970 35 NLSY 1990 30 25 Prevalence (%) 20 15 10 5 0 1 - 2 2 - 3 3 - 4 4 - 5 > 5 0 - 1 TV hours per day (youth report) Prevalence of Obesity by Hours of TV per Day NHES Youth Aged 12 to 17 in 1967-1970 and NLSY Youth Aged 10 to 15 in 1990
Medical Complications of Obesity Idiopathic intracranial hypertension Pulmonary disease abnormal function obstructive sleep apnea hypoventilation syndrome Stroke Cataracts Nonalcoholic fatty liver disease steatosis steatohepatitis cirrhosis Coronary heart disease Diabetes Dyslipidemia Hypertension Severe pancreatitis Gall bladder disease Cancer breast, uterus, cervix colon, esophagus, pancreas kidney, prostate Gynecologic abnormalities abnormal menses infertility polycystic ovarian syndrome Osteoarthritis Phlebitis venous stasis Skin Gout
Pathogenesis of Health Problems Associated with Obesity Environment Genes Activity Food Intake Excess fat stores Diseases due to increased fat cell size & visceral fat Diseases due to increased fat mass Diabetes CVD Stigma Osteoarthritis NAFLD Sleep apnea GB Disease Cancer
BMI and Mortality by Ethnic Group The American Cancer Society Study Calle NEJM 1999;341:1097.
Relative Risk of Death by BMI Levels from the NHANES I, II, & III Surveys Flegal et al JAMA;2005:1861
Obesity Decreases Life Expectancy:The Framingham Study * Compared to a BMI 18.5-24.9 kg/m2 Peeters Ann Int Med 2003;138:24-32.
Proportion of Disease Prevalence Attributable to Obesity Diet, Nutrition and the Prevention of Chronic Diseases. Report of a Joint WHO/FAO Expert Consultation. Geneva, World Health Organization (WHO Technical Report Series, No. 916).
93.2 Men Women 54.0 42.1 40.3 27.6 21.3 15.8 8.1 11.6 5.0 6.7 4.3 2.9 2.2 4.4 1.5 1.0 1.0 1.0 Relationship Between BMI and Risk of Type 2 Diabetes Mellitus 100 75 Age-Adjusted Relative Risk 50 25 0 23 - 23.9 < 22 < 23 24 - 24.9 25 - 26.9 27 - 28.9 29 - 30.9 31 - 32.9 33 - 34.9 35 + Body Mass Index (kg/m2) Chan J et al. Diabetes Care 1994;17:961. Colditz G et al. Ann Intern Med 1995;122:481.
Nurses’ Health Study: Waist Circumference Directly Related to Risk for Type 2 Diabetes *Controlled for age, family history of diabetes, exercise, smoking, saturated fat intake, calcium, potassium, magnesium, and glycemic index. Carey et al. Am J Epidemiol. 1997;145:614.
Abdominal obesity Glucose intolerance High triglycerides Low HDL-cholesterol High blood pressure Insulin resistance Microalbuminuria Small dense LDL Inflammatory markers Thrombotic factors Endothelial dysfunction Hyperuricemia Characteristics of the Metabolic Syndrome Wannabes Full members
Abdominal Adiposity Abdominal Obesity Visceral Subcutaneous Courtesy of Steven Smith, M.D.
Subcutaneous Fat Abdominal Muscle Layer Intra-abdominal Fat Visceral Adiposity:The Critical Adipose Depot
Metabolic Syndrome: NCEP ATP III compared to IDF * requires presence of 3 or more criteria ** requires central adiposity and presence of 2 more criteria
Age-Adjusted Prevalence of the Metabolic Syndrome Among 8814 Adults Age > 20 Ford JAMA 2002;287:356-9.
Mortality from Cancer in American Men and Women Calle NEJM 2003;348:1625.
Other Increased Risks • Kidney stones • Complications of pregnancy • Sleep disorders • Osteoarthritis • Stigmatization
The Interheart Study: Risk of MI * Adj for Age, Sex & Geography + Adj Age, Sex & Smoking Yusuf et al Lancet 2004;364-352.
BMI and Physical Functioning (SF-36)The Nurses Health Study Coakley et al IJO 1998;22:958-963.
Psychosocial Status of Obese Individuals • Most obese individuals have normal psychological status • Persons who seek weight loss report greater distress • Patients at greatest risk of depression: • Women • Extreme obesity (BMI ≥ 40 kg/m2) • Binge eating disorder (BED) Friedman & Brownell. Psych Bull 1995;117:3-20.
Risk of Major Depression with Extreme Obesity Onyike, et al. Amer J Epidemiology 2003;158:1139-1147.
Bodily Pain and Depression in Obese Individuals (N = 306) Bodily Pain: BDI-II Score Fabricatore AF. Obes Surg 2005; 15:304-309.
Medical Benefits of Modest Weight Loss • Reduces mortality • Lowers conversion rate to diabetes • Improves blood pressure • Reduces risk factors for CHD • Lowers lipids • Improves sleep apnea
40 30 20 10 0 0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 Diabetes Prevention Program Placebo Metformin Lifestyle Cumulative Incidence of Diabetes (%) Year Diabetes Prevention Program Research Group. N Engl J Med. 2002;346,393-403.
Small Weight Losses Are Beneficial The Diabetes Prevention Program + Placebo Reduces Risk of Diabetes by 58% Lifestyle 0 6 12 18 24 30 36 42 48 Months in study DPP NEJM 2002;346:393-402
0.02 0.5 0.0 0.00 -0.5 -0.02 -1.0 -1.5 -0.04 -2.0 -0.06 -2.5 Plasma Lipids Improve With Weight Loss Meta-analysis of 70 Clinical Trials HDL-C (weight stable) HDL-C (actively losing) Total Cholesterol LDL-C TG * * * D mmol/L per kg of Weight Loss * D mg/dL per kg of Weight Loss * *P0.05. LDL-C=low density lipoprotein cholesterol; HDL-C=high-density lipoprotein cholesterol; TG=triglycerides. Dattilo et al. Am J Clin Nutr 1992;56:320.
Effect of Weight Change on Apnea-Hypopnea Index (AHI) 6 4 2 Mean Change in AHI (Events/h) 0 -2 -4 +10 to +20 (n = 79) -20 to < -10 (n = 22) -10 to < -5 (n = 39) -5 to < +5 (n = 371) +5 to < +10 (n = 179) Change in Body Weight (%) Peppard et al. JAMA 2000;284:3015.
Economic Burden of Obesity Similar to Other Chronic Diseases Direct cost of chronic diseases in the U.S. ($2003) Billions, $ Obesity 1 75.0 Type 2 Diabetes* 2 73.7 Coronary heart disease 3 52.4 Hypertension 4 28.2 Arthritis 5 23.9 Breast Cancer 6 7.1 1Finkelstein EA, Obes Res 2004;124Hodgson TA et al. Med Care 2001;39:599 2ADA Diabetes Care, 2003;26:9175Yelin & Callahan. Arthritis Rheum 1995;38:1351 3Hodgeson TA et al. Medical Care 1999:37:994. 6Brown ML, et al. Medical Care; 2002;40(suppl): IV- 104 Courtesy of Anne Wolf, MS, RD
2.3% - Cost increase for each higher BMI unit 52.9% - Cost increase for each major associated co-morbidity Cost Difference Raebel, M. et al. Health Services Use and Health Care Costs of Obese and Non-obese Individuals. Arch Intern Med 2004; No.19. Vol.164: 2135-2140. Oct.25,2004
Obesity Effect on Expected Lifetime Medical Care Costs in Women 40,000 30,000 Costs ($) 20,000 55 -64 10,000 45 - 54 Age 35 - 44 0 37.5 32.5 27.5 22.5 BMI (kg/m2) *Total cost of 8 diseases: CHD, type 2 DM, hypertension, hypercholesterolemia, stroke, gallbladder disease, osteoarthritis of knee, endometrial cancer. Adapted from Thompson D et al. Arch Intern Med 1999;2177-2183.
Expected Lifetime Medical Care* Savings of Sustained 10% Weight Loss by Age and Initial BMI (Women) 6000 5000 4000 Costs ($) 3000 55 - 64 2000 45 - 54 1000 Age 35 - 44 0 37.5 32.5 27.5 BMI (kg/m2) *Total cost of 5 diseases: CHD, type 2 DM, hypertension, hypercholesterolemia, and stroke. Adapted from Oster G, et al. Am J Public Health 1999;89:1536-1542.
Childhood/Adolescent Health Costs • $9 – $20: Cost of a single day of absenteeism for a student • 9 days: Median # sick days away from school for the most overweight students • Obesity associated annual hospital costs for children and youth more than tripled over the last two decades • $35 million in1979 – 1981 • $127 million in 1997 – 1999 Action for Healthy Kids- The Learning Connection- Value of Improving Nutrition and Physical Activity in Our Schools. Preventing Childhood Obesity: Health in the Balance. 2005. Institute of Medicine. Childhood Obesity Prevention Study.
Obesity Medications • Obesity medications produced substantial weight loss • Drug cost savings for obesity co-morbid conditions • Subjects were taking medications for: • Diabetes • Hyperlipidemia • Hypertension • Pharmaceutical cost computed for: • Weight loss • Cardiac risk reduction • Lipid reduction • Glucose reduction Greenway, FL.. Ryan, DH. Bray, GA. Pharmaceutical Cost Savings of Treating Obesity with Weight Loss Medications. Obesity Research. 1999; 7: 523-531.
Conclusions • Obesity is a growing epidemic in the United States and worldwide • The prevalence of type 2 diabetes and obesity in children/adolescents has dramatically increased • The risk of comorbid conditions increases as obesity increases. • The economic burden of obesity is great, and increases as obesity increases