Download
1 / 1
10 likes | 90 Views
patient. age. first treatment (time before start of immunotherapy). current disease stage. serum PSA at day –2 (in ng/ml). PSA-response & duration. ELISPOT- response. #1. 57. RAD (‑3 m). OS‑MS. 10.98. NR. NR. CD86/CD80 : mono (0,39%) iDC (0,87 %) mDC (88,97%). CD80.

E N D
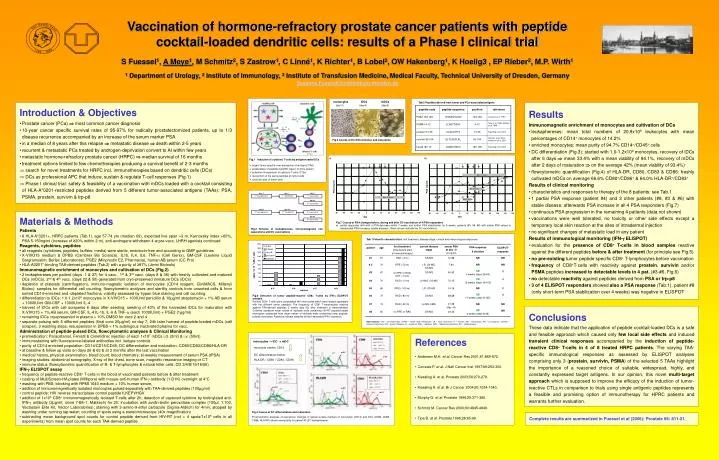
patient age first treatment (time before start of immunotherapy) current disease stage serum PSA at day –2 (in ng/ml) PSA-response & duration ELISPOT- response #1 57 RAD (‑3 m) OS‑MS 10.98 NR NR CD86/CD80: mono (0,39%) iDC (0,87 %) mDC (88,97%) CD80 CD86 Vaccination of hormone-refractory prostate cancer patients with peptide cocktail-loaded dendritic cells: results of a Phase I clinical trial S Fuessel1, A Meye1, M Schmitz2, S Zastrow1, C Linné1, K Richter1, B Lobel2,OW Hakenberg1, K Hoelig3 , EP Rieber2, M.P. Wirth1 1 Department of Urology, 2 Institute of Immunology, 3 Institute of Transfusion Medicine,Medical Faculty, Technical University of Dresden, Germany Susanne.Fuessel@uniklinikum-dresden.de # 2 70 RPE (‑72 m) LR, LN‑MS, OS‑MS 7.94 NR NR mono mDC iDC iDC mDC #3 67 no RPE or RAD, CHT (‑14 m) OS‑MS 45.93 SD 5 weeks (days 26-64) R mono CD14/-: mono (90,11%) iDC (72,64 %) mDC (8,35%) CD14 #4 70 RAD (‑13 m) LN‑MS, OS‑MS 70.15 PR 12 weeks (days 19-105) R mDC iDC mono HLA-DR / CD83: mono (0,27%) iDC (1,45 %) mDC (85,72%) HLA-DR CD83 #5 65 RPE (‑100 m) LR, OS‑MS 14.16 NR R #6 73 RAD (‑80 m) OS‑MS 68.68 SD 17 weeks (days 8-125) R mDC iDC mono mDC iDC mono #7 74 RAD (‑22 m) no MS (cM0) 21.28 (day –8) NR NR #8 65 no RPE or RAD OS‑MS 24.22 SD 4 weeks (days 8-36) NR day -1 day 0 day 8 1st leukapheresis 1st CliniMACS 1st vaccination day 22 2nd vaccination day 27 day 28 day 36 2nd leukapheresis 2nd CliniMACS 3rd vaccination day 50 4th vaccination monocytes iDCs mDCs (day 0) (day 6) (day 8) Fig.2 Scheme of leukaphereses, immunomagnetic cell separations and DC vaccinations Fig.3 Course of DC differentiation and maturation • monocytes iDC mDC monocyte marker CD14 DC differentiation marker HLA-DR / CD80 / CD83 / CD86 a) b) Fig.4 Course of DC differentiation and maturation Flowcytometric analyses of expression changes of typical surface markers of monocytes (CD14) and DCs (CD80, CD83, CD86, HLA-DR) shown exemplarily for patient #3 (2nd leukapheresis). Tab.1Patient’s characteristics: first treatment, disease stage, clinical and immunological responses Fig.6Detection of tumor peptide-reactive CD8+ T‑cells by IFN‑g ELISPOT analysis Purified CD8+ T‑cells were coincubated with monocytes which were loaded separately with the different tumor peptides. The frequency of CD8+ T‑lymphocytes reactive against TAA-derived peptides 2 weeks (day 63) after treatment is demonstrated. Columns represent mean values of triplicate wells containing HIV-RT peptide-loaded monocytes subtracted from mean values of triplicate wells containing tumor peptide-pulsed monocytes. Asterisks indicate samples without detectable IFN‑g-secretion. * * * * * * * * * * * * * abbreviations: CHT – chemotherapy, LN‑MS – lymph node metastases, LR – local recurrence, m – months, MS – metastases, NR – no response, OS‑MS – osseous metastases, PR – partial response, R – response, RAD – radiation, RPE – radical prostatectomy, SD – stable disease Tab.2 Peptides derived from tumor and PCa-associated antigens • Introduction & Objectives • Prostate cancer (PCa) most common cancer diagnosis • 10‑year cancer specific survival rates of 95-97% for radically prostatectomized patients, up to 1/3 disease recurrence accompanied by an increase of the serum marker PSA • in a median of 8 years after this relapse metastatic disease death within 2-5 years • recurrent & metastatic PCa treated by androgen-deprivation convert to AI within few years • metastatic hormone-refractory prostate cancer (HRPC) median survival of 16 months • treatment options limited to few chemotherapies producing a survival benefit of 2-3 months • search for novel treatments for HRPC incl. immunotherapies based on dendritic cells (DCs) • DCs as professional APC that induce, sustain & regulate T‑cell responses (Fig.1) • Phase I clinical trial: safety & feasibility of a vaccination with mDCs loaded with a cocktail consisting of HLA-A*0201-restricted peptides derived from 5 different tumor-associated antigens (TAAs): PSA, PSMA, prostein, survivin & trp‑p8 • Results • Immunomagnetic enrichment of monocytes and cultivation of DCs • leukaphereses: mean total numbers of 20.9x109 leukocytes with mean percentages of CD14+ monocytes of 14.2% • enriched monocytes: mean purity of 94.7% CD14+/CD45+ cells • DC differentiation (Fig.3): started with 1.0‑1.2x109 monocytes, recovery of iDCs after 6 days mean 33.4% with a mean viability of 94.1%, recovery of mDCs after 2 days of maturation on the average 42% (mean viability of 93.4%) • flowcytometric quantification (Fig.4) of HLA-DR, CD80, CD83 & CD86: freshly cultivated mDCs on average 66.6% CD80+/CD86+ & 64.0% HLA-DR+/CD83+ • Results of clinical monitoring • characteristics and responses to therapy of the 8 patients: see Tab.1 • 1 partial PSA response (patient #4) and 3 other patients (#8, #3 & #6) with stable disease, afterwards PSA increase in all 4 PSA responders (Fig.7) • continuous PSA progression in the remaining 4 patients (data not shown) • vaccinations were well tolerated, no toxicity or other side effects except a temporary local skin reaction at the sites of intradermal injection • no significant changes of metastatic load in any patient • Results of immunological monitoring (IFN‑g ELISPOT) • evaluation for the presence of CD8+ T‑cells in blood samples reactive against the different peptides before & after treatment (for principle see Fig.5) • no pre-existing tumor peptide specific CD8+ T‑lymphocytes before vaccination • frequency of CD8+T‑cells with reactivity against prostein, survivin and/or PSMA peptides increased to detectable levels in 4 pat. (#3-#6, Fig.6) • no detectable reactivity against peptides derived from PSA or trp‑p8 • 3 of 4 ELISPOT responders showed also a PSA response (Tab.1), patient #8 (only short-term PSA stabilization over 4 weeks) was negative in ELISPOT • Fig.1 Induction of cytotoxic T-cells by antigen-loaded DCs • organ-/tumor-specific over-expression of antigens (TAA) • presentation of peptides by MHC class I on DCs (green) • activation & expansion of cytotoxic T-cells (CTLs) • recognition of the same peptides on tumor cells • cytotoxic lysis of tumor cells • Materials & Methods • Patients • 8 HLA-A*0201+, HRPC patients (Tab.1), age 57-74 yrs (median 69), expected live span >3 m, Karnovsky index >60%, PSA 5-150ng/ml (increase of ≥20% within 2 m), anti-androgens withdrawn 4 w pre-vacc, LHRH agonists continued • Reagents, cytokines, peptides • all reagents (cytokines, peptides, buffers, media) were sterile, endotoxin-free and according to GMP guidelines • X‑VIVO15 medium & DPBS (Cambrex Bio Science), IL1b, IL4, IL6, TNF‑a (Cell Genix), GM‑CSF (Leukine Liquid Sargramostim, Berlex Laboratories), PGE2 (Minprostin E2, Pharmacia), human AB serum (CC Pro) • HLA-A0201*-binding TAA-derived peptides (Tab.2) with a purity of ≥97% (Jerini Biotools) • Immunomagnetic enrichment of monocytes and cultivation of DCs (Fig.2) • 2 leukaphereses per patient (days -1 & 27) for 4 vacc., 1st & 3rd vacc. (days 8 & 36) with freshly cultivated and matured DCs (mDCs), 2nd & 4th vacc. (days 22 & 50) generated from cryo-preserved immature DCs (iDCs) • depletion of platelets (centrifugation), immuno-magnetic isolation of monocytes (CD14 reagent, CliniMACS, Miltenyi Biotec); samples for differential cell counting, flowcytometric analyses and sterility controls from unsorted cells & from sorted CD14-enriched and ‑depleted fractions, viability assessed by trypan blue staining and cell counting • differentiation to iDCs: 1.0‑1.2x109 monocytes in X‑VIVO15 + 100IU/ml penicillin & 10µg/ml streptomycin + 1% AB serum + 1000IU/ml GM‑CSF + 1000IU/ml IL‑4 • harvest of iDCs with cell scraperss 6 days after seeding; seeding of 40% of the harvested iDCs for maturation with X‑VIVO15 + 1% AB serum, GM‑CSF, IL‑4 IL‑1b, IL‑6 & TNF‑a (each 1000IU/ml) + PGE2 (1µg/ml) • remaining iDCs cryopreserved in plasma + 10% DMSO for vacc 2 and 4 • separate pulsing with 5 different peptides (final conc 20µg/ml) onday 7; 24h later harvest of peptide-loaded mDCs (cell scraper), 3 washing steps, resuspension in DPBS + 1% autologous inactivated plasma for vacc. • Administration of peptide-pulsed DCs, flowcytometric analyses & Clinical Monitoring • premedication: Paracetamol, Fenistil & Cimetidine; injection of each 1x107 mDCs i.d. (2ml) & i.v. (50ml) • immunostaining with fluorescence-labeled antibodies incl. isotype controls • purity of CD14 enriched population: CD14/CD15/CD45; DC differentiation and maturation: CD80/CD83/CD86/HLA‑DR • at baseline & follow up visits on days 26 & 63 & at 3 months after the last vaccination • medical history, physical examination, blood count, blood chemistry; bi-weekly measurement of serum PSA (tPSA) • imaging studies: abdominal sonography, X‑ray of the chest, bone scan, magnetic resonance imaging or CT • immune status (flowcytometric quantification of B- & T‑lymphocytes & natural killer cells; CD 3/4/8/19/16/56) • IFN‑g ELISPOT assay • frequency of peptide-reactive CD8+ T‑cells in the blood of vaccinated patients before & after treatment • coating of MultiScreen-HA plates (Millipore) with mouse-anti-human IFN‑g antibody (1‑D1K) overnight at 4°C • washing with PBS; blocking with RPMI 1640 medium + 10% human serum, • addition of immunomagnetically isolated monocytes pulsed separately with TAA-derived peptides (100µg/ml) • control peptide: HIV reverse transcriptase control peptide ILKEPVHGV • addition of 1x105 CD8+ immunomagnetically isolated T‑cells after 2h; detection of captured cytokine by biotinylated anti-IFN‑g antibody (2µg/ml; clone 7‑B6‑1; Mabtech) for 2h; incubation with avidin-biotin peroxidase complex (100µl, 1:100, Vectastain Elite Kit, Vector Laboratories); staining with 3‑amino-9‑ethyl carbazole (Sigma-Aldrich) for 4min, stopped by washing under running tap water; counting of spots using a stereomicroscope (40x magnification) • subtracting mean background spot counts for control peptide derived from HIV-RT (not > 4 spots/1x105 cells in all experiments) from mean spot counts for each TAA-derived peptide • Fig.7 Course of PSA changes before, during and after DC vaccination of 4 PSA responders • partial responder (#4) with a PSA decrease within 7 weeks and further PSA stabilization for 5 weeks, patients (#3, #6, #8) with stable PSA values or decelerated PSA increases (stable disease).; Black arrows indicate the DC vaccinations. Conclusions These data indicate that the application of peptide cocktail-loaded DCs is a safe and feasible approach which caused only few local side effects and induced transient clinical responses accompanied by the induction of peptide-reactive CD8+ T‑cells in 4 of 8 treated HRPC patients. The varying TAA-specific immunological responses as assessed by ELISPOT analyses comprising only 3 (prostein, survivin, PSMA) of the selected 5 TAAs highlight the importance of a reasoned choice of suitable, widespread, highly, and constantly expressed target antigens. In our opinion, this novel multi-target approach which is supposed to improve the efficacy of the induction of tumor-reactive CTLs in comparison to trials using single antigenic peptides represents a feasible and promising option of immunotherapy for HPRC patients and warrants further evaluation. • References • Andersen M.H. et al.Cancer Res 2001;61:869-872. • Correale P. et al. J Natl Cancer Inst 1997;89:293-300. • Kiessling A. et al. Prostate 2003;56:270-279. • Kiessling A. et al. Br J Cancer 2004;90:1034-1040. • Murphy G. et al. Prostate 1996;29:371-380. • Schmitz M. Cancer Res 2000;60:4845-4849. • Tjoa B. et al. Prostate 1996;28:65-69. Complete results are summarized in Fuessel et al (2006): Prostate 66: 811-21.