Download

1 / 72
880 likes | 2.36k Views
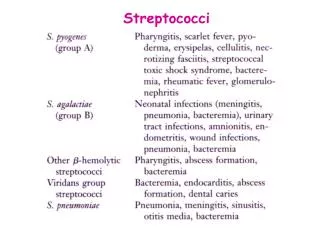
Streptococci. Streptococci. - Family: Streptococcaceae - Streptos means twisted and coiled. - Name was given by Billroth (1874) - Streptococcus pyogens name was given by Rosenbach (1884) which were isolated from suppurative lessions

E N D
Streptococci - Family:Streptococcaceae - Streptos means twisted and coiled. - Name was given by Billroth (1874) - Streptococcus pyogens name was given by Rosenbach (1884) which were isolated from suppurativelessions - Gram positive cocci which typically form chains (divide only in one plane) / pairs. - Many are part of the normal flora - Some species cause important diseases
Classification Classification is based on multiple criteria 1. Their Oxygen requirement 2. Hemolytic pattern on Sheep blood agar 3. Antigenic characteristics 4. Biochemical properties
Streptococci O2 requirement Aerobes, Obligate anaerobes Facultative anaerobes Eg: Peptostreptococcus 1.Alpha hemolytic 2.Beta hemolytic 3. Non hemolytic Partial hemolysis Complete hemolysisEg: Enterococcus (Greenish discoloration) (Clear zone) Eg: Viridans Streptococci,
Beta hemolytic Streptococci Lancefield Grouping Based on group specific “C” carbohydrate antigen 20 Lancefield Groups -> A – H & K – v Group A Streptococcus Serotyping, Based on specific “M” Protein (150 types) Griffith’s typing Griffith’s types
Group A Streptococcus(Streptococcus pyogenes,Flesh eating bacteria) Morphology - Gram positive cocci - Catalase negative - Non motile - Spherical to oval in shape -0.5-1 µm in diameter - Arranged in chains - Aerobic , Facultative Anaerobic - Optimum temp. 37⁰c (22-42⁰c) -Grow only in media containing blood, sugar or serum
Bacterial virulence factors:- Virulence factors of Streptococcus pyogenes may be divided into two categories – - Cellular virulence factors - Extracellular virulence factors
Antigenic structure: 1.Capsular hyaluronic acid: 2.Cell wall antigens: a) Inner layer of peptidoglycan b) Middle layer of group specific C carbohydrate c) Outer layer of protein (fimbriae) & lipoteichoic acid 3.Type specific antigens: a) M protein b) T protein c) R protein
Antigenic structure Toxins and Enzymes Capsule(hyaluronic acid) Inhibits phagocytosis Peptidoglycan cell wall Cell wall rigidity , Thrombolytic, Pyrogenic Fimbrial antigen and M protein Inhibits phagocytosis adherence factor’ Lipoteichoic acid Attachment to epithelial cells
Cross reacting Antigens Various streptococcal Ags have similarity to different host tissues • Capsular hyaluronic acid <–>human synovial fluid • Cell wall M protein <–>myocardium • Cytoplasmic membrane antigen <–>vascular intima • These antigenic cross reactions may be responsible for the non-suppurativecomplications of group A Streptococcal infections.
Extracellular Virulence Factors Toxins - Pyrogenic exotoxins (erythrogenic toxins) A, B, C -> Highly antigenic • Pyrogenic – induce fever • Responsible for skin rashes in scarlet fever • Superantigens, responsible for streptococcal SSS • Have ability to alter lymphocytic activity
2. Streptolysins - • Hemolysins of Group A streptococcus • Two types – Streptolysin ‘O’ - Streptolysin ‘S’
Streptolysin ‘O’ • ‘O’ -> means oxygen labile, hemolytic activity • MW -> 60,000 Daltons • Active against RBC, WBC • Antigenic -> Abs raised are called Antistreptolysin O Abs (ASO) • Estimation of this antibody (ASO) titre helps in the diagnosis of streptococcal disease
Streptolysin ‘S’ • It is oxygen stable • Active against RBC, WBC, Platelets • Responsible for the Beta hemolysis seen around the colonies on the surface of blood agar • Has nephrotoxic activity
B. Enzymes of Str.pyogenes Streptokinase - • Can digest fibrin clots ( plaminogen in to plasmin) • Helps in Streptococcal infections by breaking down the fibrin barrier around the lesions and facilitating the spread of infection. • Practical use – given IV for treatment of pulmonary emboli; coronary artery/venous thromboses
Streptodornase (Streptococcal DNAse) Released by dead host cells. Responsible for the decrease in viscosity of purulent pus. Responsible for the serous nature of exudate in streptococcal infection. Help in spread of lesion. Mixture of streptokinase/streptodornase Practical use: in enzymatic debridement of necrotized tissues & empyemas . – facilitates early recovery of infected tissue
Hyaluronidase -> Spreading factor’ • Degrades hyaluronic acid , – it facilitates the rapid spread of Str. pyogenes in skin infection
Streptococcus pyogenes infections Pathogenesis - Source:- • Patients with skin lesions; respiratory secretions of sore throat cases • Carriers Mode of infection:- • Direct/Indirect contact or inhalation
Diseases: attributable to streptococcus group A Diseases caused by S. pyogens is studied under 2 groups 1. Suppurative infections 2. Non suppurative complications
Suppurative infections: Pyogenic infections. Spreads locally, along lymphatics and through the blood stream. A) Respiratory infections - Tonsillitis - Pharyngitis - Otitis media -Mastoiditis -Quinsy - Ludwig’s angina - Rarely it may cause pneumonia & meningitis - Scarlet fever (sore throat & skin rash)
Pharyngitis Tonsillitis Mastoiditis Otitis media
Quinsy Ludwig’s angina Skin rashes in Scarlet fever
B) Skin infections:- - Infection of wounds & burns - Impetigo - Erysipelas C) Soft tissue infections:- - Cellulitis - Necrotising fasciitis
Soft tissue infections with some M types of strains may sometime cause toxic shocksyndrome resembling staphylococcal TSS. D) Genital Infections:-Puerperal sepsis E) Other suppurative infections:- - Pyemia - Septicemia - Abscesses in internal organs such as brain, lungs, liver and kidney.
2. Non suppurative complications: • It is also called as post streptococcal complications • Non suppurative complications of S.pyogens occur 1-4 weeks after the acute infection. • The organism may not be detectable when these complications set in.
These complications are believed to be the result of hypersensitivity to some streptococcal components. • The complications are- 1. Acute rheumatic fever 2. Acute glomerulonephritis
Acute rheumatic fever: It occurs after (1-4 weeks ) repeated sore throat caused by S. pyogens. Mechanism of pathogenesis: Primary infection antibodies produced against some streptococcal antigen. Similarity with cardiac tissue antigen Antibodies will cross react with cardiac tissue antigen causing destruction. Leads to clinical symptoms such as Aschoff’snodules,carditis, fever and malaise.
Acute glomerulonephritis: It follows about 3 weeks after skin infection caused by S. pyogens nephritogenic types.(M types 49,55,59,61) Mechanism of pathogenesis: Antibodies will be produced against cell membrane antigen. These antibodies cross react with glomerular basement membrane antigen causing Complement mediated damage. Leads clinical symptoms such as proteinuria, haematuria & hypertension.
Comparison of Acute Rheumatic Fever and Acute Glomerulonephritis
Lab diagnosis Specimen– Collection depends on type of disease • Throat swab, • pus, • exudates, fluids • necrotic tissue–> for culture • Serum -> for serology
Methods:- Microscopy -> • Gram’s stained smear:- Gram positive cocci in long chains along with pus cells (May not be useful in case of throat swabs) • Immunofluorescent staining:- Direct immunofluorescent staining using specific monoclonal Abs – highly sensitive & specific
Culture -> • Specimen should be immediately processed • Transport media – Pike’s / Stuart’s media used if delay in processing • Routine media used – Sheep Blood agar; Thioglycollate medium • Incubated for 24-48 hrs at 37oC in 5-10% CO2
Identification of Isolate -> • Beta hemolytic colonies • Gram positive cocci in chains • Catalase test negative • Isolate is susceptible to bacitracin • Grouping (Lancefield) is done by Co-agglutination test to detect ‘Group A Streptococci’
Serology - Rise in titre of Abs to many Group A Streptococcal Ags may be demonstrated. • Antistreptolysin O (ASO) test:- • A serological test used to detect ASO Abs present in patient’s serum • A passive latex agglutination test • ASO titre of more than 200 units is indicative of recent streptococcal infection
May also indicate an exaggerated immune response to an earlier exposure (ARF) • Useful in the diagnosis of ARF but not in AGN as titre is low (usually occurs as a result of skin infection and being oxygen labile toxin, Ab will not be produced in high titre)
Other serological tests - • Antistreptodornase (AntiDNAse) test • Antihyaluronidase test • Antistreptokinase test
Treatment • Penicillin G is the drug of choice. • Patients allergic to penicillin: erythromycin / cephalexin may be used. • All acute infections should be treated, as antimicrobials have no effect on already established ARF & AGN • Long term Penicillin therapy for ARF patients to prevent recurrence of infection
Streptococcus agalactiae • It is part of the normal flora of the female genital tract (5 – 20% of women) • Human pathogenecity Neonatal infections Infections in adults
Neonatal infections • Early onset disease • Seen at birth or within 7 days of birth • Source of infection mothers birth canal • Predisposing factors • Prolonged labor • PROM • Premature child • Low birth weight • Manifestations Septicemia, meningitis, pneumonia
Late onset disease • Occurs after first week of life • Source hospital staff, environment. • Manifestation • Sepsis with /without meningitis • Respiratory tract infection
Adult infections - • In women • Abortion • Chorioamnionitis • Post partum sepsis • In debilitated individuals • Septicemia • Meningitis • Endocarditis
Lab diagnosis - • Specimen-> CSF, Blood, Exudates • Cultured onto -> Sheep Blood Agar • Incubated at -> 37o C for up to 48 hrs • Isolate identified by -> • Beta hemolysis on blood agar • Gram stained smear – Gram positive cocci in chains • Ability to hydrolyze Hippurate • CAMP test: positive
Christie Atkins Munch Petersen Test(CAMP Test) Test used to identify Group B Streptococci PrincipleEnhancement of β hemolysis of S.aureus by a soluble protein (CAMP factor) produced by Strep. Agalactiae ObservationArrow head hemolysis is seen in-between the two streaks of growth
S.aureus S.Agalactiae Group B S.Pyogens Group A Enhancement of βhemolysis
Treatment • Penicillin is the drug of choice