Download
1 / 37
370 likes | 562 Views
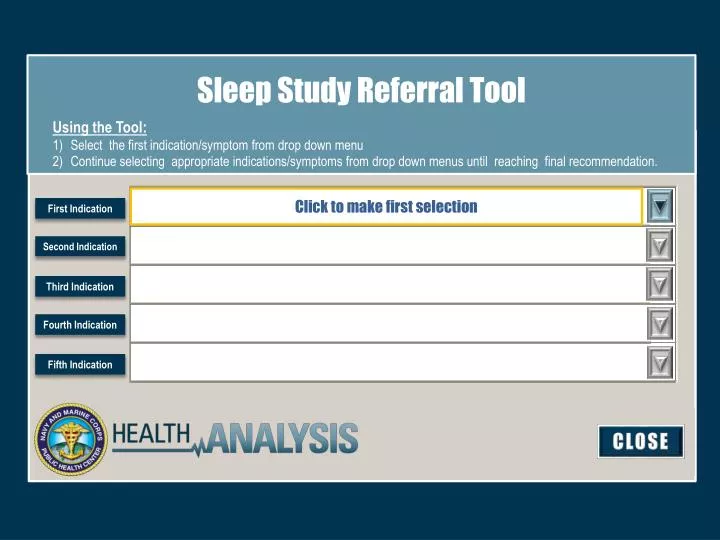
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Click to make first selection. First Indication. Second Indication.

E N D
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Click to make first selection First Indication Second Indication Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. First Indication Snoring Hypersomnia/Fatigue Witnessed Gasping as Night Second Indication Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Second Indication Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Second Indication Mild/Single Complaint Loud, Continuous for > 3 months Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Mild/Single Complaint Second Indication No referral necessary Provide conservative measures. Third Indication NEXT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Conservative Measures: Avoid ETOH at night Consider lateral positional sleeping Consider OTC* sleep wedge pillow Consider Flonase for nasal congestion – treat allergic rhinitis Consider OTC* extra strength nasal strips Smoking Cessation OTC* = over the counter Patient will need to purchase item. Item is not a Tricare benefit Mild/Single Complaint Second Indication Third Indication EXIT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Loud, Continuous for > 3 months Second Indication Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Loud, Continuous for > 3 months Second Indication Third Indication ESS > 15 OR STOP-BANG > 5? Determine BMI. Is BMI > 25? Determine BMI. Is BMI < 25? Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Loud, Continuous for > 3 months Second Indication Sleep Medicine Referral ESS > 15 OR STOPBANG > 5? Third Indication EXIT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Loud, Continuous for > 3 months Weight loss recommended > 10% OR until BMI is < 25 Provide conservative measures. Second Indication Determine BMI. Is BMI > 25? Third Indication NEXT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Conservative Measures: Avoid ETOH at night Consider lateral positional sleeping Consider OTC* sleep wedge pillow Consider Flonase for nasal congestion – treat allergic rhinitis Consider OTC* extra strength nasal strips Smoking Cessation OTC* = over the counter Patient will need to purchase item. Item is not a Tricare benefit Loud, Continuous for > 3 months Second Indication Determine BMI. Is BMI > 25? Third Indication EXIT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Loud, Continuous for > 3 months Second Indication Determine BMI. Is BMI < 25? Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Loud, Continuous for > 3 months Second Indication Determine BMI. Is BMI < 25? Third Indication Fourth Indication Provide Conservative Measures. Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Snoring First Indication Conservative Measures: Avoid ETOH at night Consider lateral positional sleeping Consider OTC* sleep wedge pillow Consider Flonase for nasal congestion – treat allergic rhinitis Consider OTC* extra strength nasal strips Smoking Cessation OTC* = over the counter Patient will need to purchase item. Item is not a Tricare benefit Loud, Continuous for > 3 months Second Indication Determine BMI. Is BMI < 25? Third Indication Provide Conservative Measures. EXIT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Second Indication Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Second Indication Obtain ESS Score. Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Obtain ESS Score. Second Indication Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Obtain ESS Score. Second Indication Third Indication Is ESS > 15 with sleep time > or = 7 Hours? Is ESS > 15 with sleep time < 7 Hours? Is ESS < 15 with sleep time < 7 Hours? Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Obtain ESS Score. Second Indication Sleep Medicine Referral Is ESS > 15 with sleep time > or = 7 Hours? Third Indication EXIT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Obtain ESS Score. Second Indication Assess for adequate sleep And educate on sleep habits Is ESS > 15 with sleep time < 7 Hours? Third Indication NEXT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Better Sleep Habits: If total sleep time < 7 hours then increase by 1 hour. Review all medications. Screen for depression. Obtain Sleep Diary. Provide tips on minimizing sleepiness (shift work). Consider screening labs. Obtain ESS Score. Second Indication Is ESS > 15 with sleep time < 7 Hours? Third Indication Fourth Indication EXIT NEXT Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Screening Labs: Thyroid Function Tests (TFTs) Complete Blood Count (CBC) test Basic Metabolic Panel (BMP) lab Ferritin levels Obtain ESS Score. Second Indication Is ESS > 15 with sleep time < 7 Hours? Third Indication NEXT EXIT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Obtain ESS Score. Second Indication Assess for adequate sleep And educate on sleep habits Is ESS < 15 and sleep time < 7 Hours? Third Indication NEXT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Better Sleep Habits: If total sleep time < 7 hours then increase by 1 hour. Review all medications. Screen for depression. Obtain Sleep Diary. Provide tips on minimizing sleepiness (shift work). Consider screening labs. Obtain ESS Score. Second Indication Is ESS < 15 and sleep time < 7 Hours? Third Indication Fourth Indication EXIT NEXT Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Hypersomnia/Fatigue First Indication Screening Labs: Thyroid Function Tests (TFTs) Complete Blood Count (CBC) test Basic Metabolic Panel (BMP) lab Ferritin levels Obtain ESS Score. Second Indication Is ESS > 15 with sleep time < 7 Hours? Third Indication NEXT EXIT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Second Indication Use Differential Diagnosis of Nocturnal Respiratory Symptoms Third Indication Fourth Indication NEXT Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Second Indication Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Second Indication Evaluate for possible underlying Cardiac or Pulmonary conditions. Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Evaluate for possible underlying Cardiac or Pulmonary conditions. Second Indication Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Evaluate for possible underlying Cardiac or Pulmonary conditions. Second Indication Third Indication If positive/suspicion consider referral to Cardiology or Pulmonary. If negative/unlikely administer STOP-BANG Questionnaire. Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Evaluate for possible underlying Cardiac or Pulmonary conditions. Second Indication Sleep Medicine Referral If positive/suspicion consider referral to Cardiology or Pulmonary. Third Indication EXIT Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Evaluate for possible underlying Cardiac or Pulmonary conditions. Second Indication If negative/unlikely administer STOP-BANG Questionnaire. Third Indication Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Evaluate for possible underlying Cardiac or Pulmonary conditions. Second Indication If negative/unlikely administer STOP-BANG Questionnaire. Third Indication Fourth Indication STOP-BANG Results: 3 or More STOP-BANG Results: Less than 3. Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Evaluate for possible underlying Cardiac or Pulmonary conditions. Second Indication Sleep Medicine Referral If negative/unlikely administer STOP-BANG Questionnaire. Third Indication EXIT EXIT STOP-BANG Results: 3 or More Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Evaluate for possible underlying Cardiac or Pulmonary conditions. Weight loss recommended > 10% OR until BMI is < 25 Provide conservative measures. Second Indication If negative/unlikely administer STOP-BANG Questionnaire. Third Indication NEXT STOP-BANG Results: Less than 3 Fourth Indication Fifth Indication CLOSE
Sleep Study Referral Tool Using the Tool: Select the first indication/symptom from drop down menu Continue selecting appropriate indications/symptoms from drop down menus until reaching final recommendation. Witnessed Apnea Gasping at Night First Indication Conservative Measures: Avoid ETOH at night Consider lateral positional sleeping Consider OTC* sleep wedge pillow Consider Flonase for nasal congestion – treat allergic rhinitis Consider OTC* extra strength nasal strips Smoking Cessation OTC* = over the counter Patient will need to purchase item. Item is not a Tricare benefit Evaluate for possible underlying Cardiac or Pulmonary conditions. Second Indication If negative/unlikely administer STOP-BANG Questionnaire. Third Indication STOP-BANG Results: Less than 3 EXIT Fourth Indication Fifth Indication CLOSE