Download

1 / 32
320 likes | 723 Views
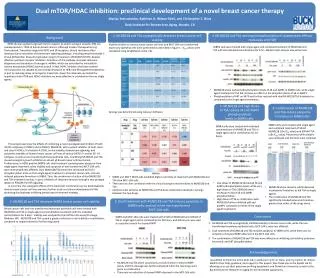
PARP Inhibition: A New Approach To Cancer Therapy? Dr. Geert Kolvenbag. Potential Conflict of Interest. Employee and Shareholder / 1988 - AstraZeneca. PARP Inhibition: A New Therapeutic Approach?. Geert J.C.M. Kolvenbag MD PhD Global Product Vice President AstraZeneca. Why is DNA

E N D
PARP Inhibition: A New Approach To Cancer Therapy?Dr. Geert Kolvenbag
Potential Conflict of Interest • Employee and Shareholder / 1988 - • AstraZeneca
PARP Inhibition:A New Therapeutic Approach? Geert J.C.M. Kolvenbag MD PhD Global Product Vice President AstraZeneca
Why is DNA repair a good target? Targeting DNA Repair in Oncology DNA damage occurs all the time in all cells DNA repair defects lead to increased cancer susceptibility and increased sensitivity to DNA damaging agents Normal cells have multiple DNA repair pathways but some are lost in cancer cells Inhibiting DNA repair in cancer cells that have impaired repair pathways leads to selective cell killing and an increased therapeutic ratio
Pre-cancerous Cell Normal Cell DNA damage leads to continuous activation of pathway A Full complement of repair pathways AB AB Cancer Cell Selective pressure loss of pathway A, genetic instability, reliance on pathway B AB B AB Alternative DNA repair pathways available Pathway B inhibitor Death Survival B Inducing Synthetic Lethality in Cancer Cells
Cancer Cells are Highly Susceptible to DNA Repair Inhibition • Cancer cells • Undergo deregulated proliferation • less time for DNA repair than in normal cells • Grow under stress, which causes ongoing DNA damage • Have DNA repair defects • mutator phenotype • allow growth despite ongoing genome instability • Are reliant on the DNA repair pathways they still retain
Type of damage: Single- strand breaks(SSBs) Bulky adducts O6- alkylguanine Insertions & deletions Mismatch repair Base excision repair Repair pathway: Nucleotide- excision repair Directreversal Repair enzymes: PARP XP, poly-merases AGT MSH2,MLH1 Focus on DDR Pathways for SSBs/DSBs Double- strand breaks(DSBs) Recombinational repair HR NHEJ ATM BRCA DNA-PK
PARP olaparib SSBs increased by dacarbazine, temozolomide and topotecan Replicating cells DSBs increased by platinums Normal cell Cancer cell with HRD Repair by Homologous Recombination No effective repair(No HR pathway) Survival Cell death Mechanisms of Action of Olaparib Mechanism 2: Potentiation Mechanism 1: Tumor specific killing by olaparib
Hypothesis • In situations where the DNA repair is compromised inhibition of PARP will lead to synthetic lethality of the cell • DNA repair factors deficient in functioning: • BRCA gene deficient in genotype or phenotype • Other Homologues Recombination Repair factors deficient in functioning (HRD) , eg ATM, MDC1, MRE11 • In presence of DNA damaging agents • Chemotherapy • Radiotherapy
IC50 on PARP-1 = 4.9 nM IC50 on PARP-2 ≈ 5nM IC50 on PARP-3 ≈ 50nM IC50 on Tankyrase >1M Olaparib: An oral inhibitor ofPoly (ADP-ribose) Polymerase (PARP) • olaparib (AZD2281; KU-0059436) • Favorable PK • Good bioavailability across species • Tumor PK -Significant levels at 24 hrs following single oral dose
Does the PARP inhibition result in therapeutic effects • In vitro • In vivo • Clinical response
BRCA2+/+ BRCA1+/+ BRCA2+/- BRCA1+/- BRCA1-/- BRCA2-/- Increased Sensitivity of BRCA1-/- and BRCA2-/-Cells to PARP Inhibition No difference in sensitivity between heterozygous and wild-type BRCA cells Targeted inhibition selective and less toxic therapy Farmer et al. Nature 2005; 434:917-21
BRCA 1 & 2 -/- ES Cells are Very Sensitive to PARP Inhibition Log surviving fraction 0 Increased levels of chromosomal aberrations in PARP inhibitor treated BRCA2 -/- cells - 1 4 Complex aberrations 3 - 2 Mean number of chromatid aberrations per cell Wild type Chromatid breaks 2 BRCA2 +/- - 3 BRCA2 -/- 1 - 4 0 10-9 10-8 10-7 10-6 10-5 10-4 0 PARP inhibitor concentration (M) WT WT + PARPi BRCA-/- BRCA2-/- + PARPi Farmer et al. Nature 2005; 434:917-21
KU95 Cell Line Panel: Olaparib Sensitivity Olaparib IC data by tumor type 50 RAD51 DNA damage induced foci HRD and Sensitive HR Proficient and Resistant
TN Breast BRCA FANC FANC ATM MDC1 Serous Ovarian BRCA Head & Neck NSCLC CRC ATM /MRE11 ATM /MRE11 MRE11 MDC1 HRD is Strongly Linked with Cancer Breast Ovarian H&N NSCLC GI, HCC Pancreas Paediatrics Mre11 ATM BRCA1 BRCA2 CHK2 MDC1 ATM BRCA1 Mre11 BRCA2 Mre11 ATM MDC1 Mre11 BRCA2 BRCA1
CFA Analysis of Breast Cancer Lines using Olaparib 25 cell lines from the Slamon breast cancer panel Alan Lau; Richard Finn & Dennis Slamon
%Sensitive (< 1µM) %Sensitive (< 1µM) %Sensitive (< 1µM) %Sensitive (< 1µM) %Insensitive %Insensitive %Insensitive %Insensitive Response to Olaparib by HR Status Triple Negative cell lines (n=14) HRD (n=12) 25.00 43.75 56.25 75.00 ER-, PR -, Her2+ cell lines (n=11) HR proficient (n=13) 0.00 22.22 77.78 100.00
Olaparib Inhibits Growth of HRD Tumors in vivo Aaron Cranston (KuDOS) & Richard Finn (UCLA)
Olaparib in Spontaneous BRCA2-Deficient Tumors Vehicle PARPi qdx28 i.p. 50mg/kg Mean RTV day 28 = 15.3 Mean RTV day 28 = 1.20 BRCA2-deficient KO Mice
From Targeted Therapy to the Olaparib Phase I Study • Oral, small molecule PARP inhibitor • IC50 for PARP1 enzyme in the low nM range • Phase I trial began at RMH then NKI; later expanded to other centres • Escalation phase: All tumor types • Primary objectives of safety and tolerability • Expansion phase: BRCA mutation carriers (HR deficient) especially ovarian cancer • Further assessment of efficacy
Overall Recruitment • Escalation Phase (n=46)1,2 • Various tumor types; BRCA carrier status not mandatory • 10 dose level cohorts: • 10mg daily given for 2 out of 3 weeks • 600mg bid continuous dosing • 11 BRCA carrier ovarian cancer • Expansion phase (n=52) at 200mg bid continuous2 • Confirmed BRCA mutation carriers • 39 ovarian cancer 1Fong et al. Proceedings of ASCO 2006 2Yap et al. Proceedings of ASCO 2007
Toxicitiesfirst 60 patients, all tumor types) • Most toxicities were Grade 1-2 (≥95%) • Most common toxicities were: • nausea 28%, vomiting 18%, dysgeusia 13%, anorexia 12% • fatigue 28% • Grade 3-4 toxicities were rare: • myelosuppression (≤5%) • nausea and vomiting (2-3%) • CNS: dizziness or mood changes (2-3%) • Pattern of toxicity similar in BRCA mutation carriers
Dose Limiting Toxicities (DLT) Maximum Tolerated Dose (MTD) = 400mg bid
Platinum Sensitivity Correlated with Response to Olaparib Resistant Sensitive Refractory Platinum-free interval (months) CR/PR SD >4 months PD
Ovarian BRCA1-/- 12 mm 6.8 mm Breast BRCA? 21.05.07 03.04.07 3 mm 6.5 mm
Olaparib Resistance • Pre-clinical • Over expression of pgp (olaparib is pgp substrate) • Reactivating BCRA mutation • Clinical • Todate no evidence of PARP inhibitor resistence • Note: Platinum resistence has been shown due to reactivating BRCA mutation
Olaparib Overcoming Drug Resistance • Pre-clinical • Overcome TMZ resistence • Potentiation of chemotherapy, e.g. TMZ • Clinical • No data yet
Summary • AZD2281 is a potent inhibitor of PARP and has impressive clinical activity in BRCA patients with breast and ovarian cancer • The drug has additional potential to benefit a larger group of patients with HRD tumors • Patient selection is key to the success of this project and is a paradigm for personalized health care • The development of biomarkers and a diagnostic are complex but pivotal to: Delivery of the right drug, at the right dose to the right patient
Acknowledgements • The patients and their families • Royal Marsden Hospital • Janet Hanwell • Dimitrios Magkos • Netherlands Cancer Institute • Jana van der Sar • Marja Voogel • Edinburgh Cancer Centre • UZ Brussel Oncologisch Centrum • International Hereditary Cancer Centre, Poland • Jan Lubinski • Cancer Research UK • Institute of Cancer Research/ Breakthrough Breast Cancer Research UK • Andrew Tutt • Pei-Jun Wu • Alan Ashworth • AstraZeneca • John Stone • Mark O’Connor • Helen Swaisland • Peter Mortimer • Jim Carmichael • Clinical teams • Theradex UK • FECS/AACR/ASCO Methods in Clinical Cancer Research Workshop, Flims, 2005