Download
1 / 26
260 likes | 651 Views
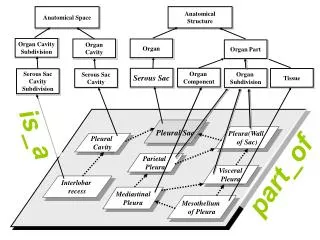
Pleural Diseases. Anatomy of the Pleura (embryology). The Pleural cavity derivatives are derived from splitting of the lateral mesoderm into splanchnic and somatic layers. The paired cavities are separated by 3 partition into 3 subdivision: Pericardial, Pleural, and Peritoneal cavity

E N D
Anatomy of the Pleura (embryology) • The Pleural cavity derivatives are derived from splitting of the lateral mesoderm into splanchnic and somatic layers. • The paired cavities are separated by 3 partition into 3 subdivision: Pericardial, Pleural, and Peritoneal cavity • The three partition are: The Unpaired septum transversum, the Paired pleuropericardial folds, the Paired pleuroperitoneal folds
Anatomy of the Pleura (histology) • Submesothelial layer contains collagen tissue, elastic fiber, small blood vessels, lymphatic network, nerve fiber. The cell in this layer is fibroblast, negative of cytokeratin, carcinoembryonic antigen, factor VIII-related antigen. • The parietal pleura has large dehiscence or stomata, connecting the pleural cavity with subpleural lymphatic network and permit entrance of material into the lymphatics from the pleural space
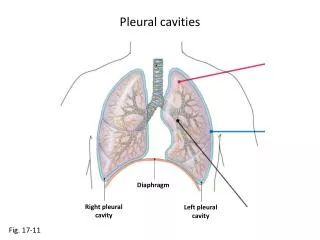
Anatomy of the Pleura (gross anatomy) • The parietal pleura lines the chest wall, mediastinum, diaphragm, and form the cupola or pleura dome at the thoracic inlet bilaterally. • The diaphragmatic pleura adheres tightly to the diaphragm. The mediastinum pleura adherent tightly to pericardium. The cupola, costal pleura can dissected from the underlying tissue. • The pleura recesses, usually two, is visible at chest PA i.e. the Azygoesophageal recess and the Superior esophageal recess
Anatomy of the Pleura (Blood supply) • Visceral pleura arterial supply is from the bronchial and pulmonary arterial systems. • The veinous drainage is to the Pulmonary veins. • The parietal pleura arterial supply is from various systemic arterial supply of the chest wall, diaphragm, and mediastinum. • Veinous drainage is directly is to the superior vena cava.
Anatomy of the Pleura (Lymphatics) • The lymphatic drainage of the visceral is to the pulmonary plexus located in the interlobar and peribronchial space. A direct subplerual lymphatic connection to mediastinal node is possible in 22-25% of people. • Lymphatic drainage of the parietal pleural is to the parietal pleural lymphatic channels, the stomata and around the Kampmeier’s foci. The lymphatic network of the chest wall drain into internal mammary chain anteriorly and intercostals chain posteriorly. The drainage of the diaphragmatic pleura is to retrosternal and mediastinal and celiac lymph node
Anatomy of the Pleura (Nerve supply) • Parietal pleura is innervated by both somatic, sympathetic and parasympathetic fiber via the intercostal nerve. • The diaphragmatic pleura is supplied by phrenic* nerve. • The visceral pleura is devoid of any somatic nerve supply.
Important points of note • Under normal condition the pleura cavity and spaces contains no free air. • The virtual space between the parietal and visceral pleura is under negative pressure in relation to the surrounding outside air.
Laws of the pleura gas exchange The rate of gas resorption in the pleural spaces are depends on four laws: 1) Diffusion properties of the gas. 2) The pressure gradient for the gas in pleura in relation to venous blood. 3) The area contact between pleura gas and pleura. 4) Permeability of the pleural surface. Ex: the oxygen is resorbed 62 times faster than nitrogen, CO2 23 times more soluble than O2. water and CO2 share the same equilibrum.
Pneumothorax Is the collection of air or gas in the pleural cavity of the chest between the lung and the chest wall. Clinical subtypes • Spontaneous Pneumothorax (COPD > 70 %, emphysema & cystic fibrosis) • Traumatic Pneumothorax (blunt injury) • Tension Pneumothorax
3 potential situations may affect the resorptibility of air causing a Pneumothorax • Close rigid cavity: Non re-expandable lung. • Closed collapsible cavity: Due to a negative intrapleural pressure. • Open cavity*: the communication between the lungs, pleural cavity, and chest wall (Bronchopleural fistula)
Pleural Masses • Benign: Lipomas, & pleural fibromas, and rounded atelectasis. • Malignant: Metastasis* (most common), other less common causes Lymphoma, thymomas & asbestos related Malignant mesothelioma
39-year old female with no significant past medical history Benign pleural fibroma
Usually found incidentally by chest radiography • Common in 4th to 6th decade, +/- hx of asbestos exposure, no gender distribution. • Presenting symptoms (~50-60% asymptomatic),others symptoms (dyspnea, chest pain, hemoptysis). • Most behave as slowly growing, painless masses. Associated hypertrophic pulmonary osteoarthropathy and episodic hypoglycaemia (due to production of insulin-like growth factor) may be present in 4-5% of cases. • 80% arise from visceral pleura and 20% from parietal pleura. • Calcification present in ≤5%, central necrosis is common in the larger tumors.
49-year old Pxt presented with no symptoms of tightening chest pain. At presentation
A few weeks later Malignant pleural mesothelioma
Malignant pleural mesothelioma is tumor that develops from the protective lining covering the outer lining of the lungs and internal chest wall due to exposure to asbestos. • CXR may show unilateral, concentric, plaque like, or nodular pleural thickening. • CT shows in detail involvement of mediastinum and diaphragm and chest wall. • MRI shows the plagues as hyperintense < muscles on T2w.
70-year-old man patient admitted with chest pains, dyspnea, and cough Pleural lipoma
Pleural lipomas are benign soft-tissue neoplasms that originate from the submesothelial layers of parietal pleura and extend into the subpleural, pleural or extrapleural space. • Are soft, encapsulated fatty slow growing tumors. • CT may demonstrate fat attenuation (approximately -100 HU) (3). If lesion is close to diaphragm may be mistaken for a hernias (Morgagni & Bochedalek)
66-year-old asymptomatic patient with a previous history of having worked in the mine Round Atelectasis
Round atelectasis is an unusual form of lung collapse adjacent to the pleural surface & may simulate a pulmonary neoplasm • Comet tail sign* is pathognomonic & occurs due to distortion of vessels and bronchi that lead to an adjacent area of round atelectasis. Bronchovascular bundles appear to be pulled into the mass and resemble a comet tai. Comet tail sign may be appreciated on both CT and conventional X ray images. • Crow’s feet sign linear bands radiating from mass into lung parenchyma. • Linear densities radiate back toward hilum . • Air bronchogram