Download
1 / 34
420 likes | 1.19k Views
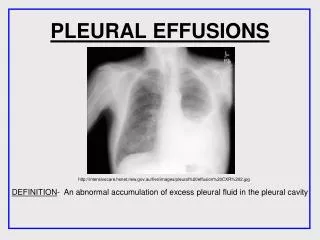
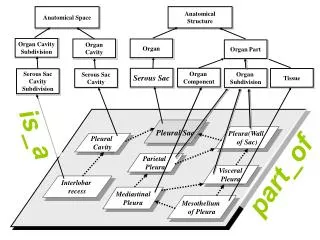
PLEURAL EFFUSIONS. Anatomy of pleural membrane and pleural space 1 234. Pleural membrane consists of parietal pleura and visceral pleura A space situated between parietal and visceral pleura is called pleural space

E N D
Anatomy of pleural membraneand pleural space 1234 Pleural membrane consists of parietal pleura and visceral pleura A space situated between parietal and visceral pleura is called pleural space It is normally filled with 5 - 10 milliter of serous fluid
Anatomy of pleural membraneand pleural space 1234 Parietal pleura Receiving its blood supply from the systemic circulation and containing sensory nerve ending
Anatomy of pleural membraneand pleural space 1234 Visceral pleura Receiving its blood supply from the low pressure pulmonary circulation and containing no sensory nerve fibers
Mechanism of formation-resorptionof pleural fluid Parietal Visceral pleura pleura Hydrostatic pressure(30) Pressure of pleural space (5) 11 Permeability of systemic circulation(34) Permeability of pleural fluid (8) 34 5+8+30-34=9 34-(5+8+11)=10
The mechanisms that lead to accumulation of pleural fluid l. Increased hydrostatic pressure in microvascular circulation(congestive heart failure) 2. Decreased oncotic pressure in microvascular circulation(severe hypoalbuminemia ) 3. Increased permeability of the microvascular circulation(pneumonia) 4. Impaired lymphatic drainage from the pleural space(malignant effusion) 5. Movement of fluid from peritoneal space( ascites )
Two kinds of pleural effusions Transudates and exudates Transudate Exudate • Cause non-inflammatory flammatory,tumor • Apperance light yellow yellow, purulent • Specific gravity <1.018 >1.018 • Coagulability unable able • Revalta test negative positive • Protein content <30g/L >30g/L • ΘP. To serum Pre < 0.5 > 0.5 • LDH < 200 I U/ L > 200 I U / L • Θ P. To s < 0.6 > 0.6 • Cell count < 100×10 6/ L > 500×10 6 / L • Differential cell Lymphocyte Different
Common causes of pleural effusions Transudates 1. Generalized salt and water retention, e.g., congestive heart failure, nephrotic syndrome, hypoalbuminemia 2. Ascites, e.g., cirrhosis, meigs' syndrome, peritoneal dialysis 3. Vascular obstruction, e.g., superior vena cava obstruction 4. Tumor
Exudates l. Infectious diseases, e.g., TB, bacterial pneumonias, and other infectious diseases. 2. Tumor 3. Pulmonary infarction 4. Rheumatic diseases
Haemorrhagic effusion l. Trauma 2. Tumor 3. Pulmonary infarction 4. TB 5. Spontaneous pneumothorax
Chylous effusion 1. Trauma 2. Tumor 3. TB 4. Thrombosis of the left subclavian vein
Empyema l. TB 2. Pulmonary infection 3. Trauma 4. Esophageal rupture
Bilateral effusion 1. Generalized salt and water retention e.g., congestive heart failure nephrotic syndrome 2. Ascites 3. Pulmonary infarction 4. Lupus erythematosus e.g., rheumatoid arthritis 5. Tumor 6. TB
T B ( Tuberculosis ) is the most common cause of pleural effusion , especially in young people Malignant pleural effusion is frequently met in aged people today Pleural transudation is most commonly caused by congestive heart failure
Diagnostic procedures1 2 3 4 5 • History(primary diseases) • clinical signs • physical examinations
clinical signs pleural pain, dyspnea, tachypnea, mild outward bulging of the intercostal spaces, decreased tactile fremitus, dullness or flatness, decreased transmission of breath and vocal sounds in the area of the effusion, and occasionally pleural friction sound in its early stage (dry pleurisy)
Diagnostic procedures1 2 3 4 5 Chest X-ray examination Blunting of the normally sharp costophyrenic angle, a concave shadow with its highest margin along the pleural surface, shift of the mediastinum and the trachus toward the normal side
Diagnostic procedures1 2 3 4 5 Ultrasonic examination To localize a small pleural effusion and determine the correct site for performance of a thoracentesis
Diagnostic procedures1 2 3 4 5 Thoracentesis To aspirate the effusion for laboratory examination: Appearance, Specific gravity, Protein content, Cell counts, Glucose, LDH lipid content, Rheumatoid factor (RF), Adenisine deaminase (ADA), Lupus pleuritis (LE) cells, Gram stain and culture, Cytologic examination, etc.
Diagnostic procedures1 2 3 4 5 Pleural biopsy To obtain a specimen for histologic examination and culture
胸腔积液诊断思路 有无胸腔积液? 胸穿抽液 漏出液? 渗出液? 分析病因 针对病因治疗
Treatment Treatment for many pleural effusions, whether transudates or exudates is primarily for the underlying pulmonary or systemic disease: aspiration of fluid is usually indicated to establish the diagnosis It is also therapeutically used to relieve dyspnea from a large effusion
Tuberculous pleural effusion • TB remains the most common cause of pleural effusion in young people • Etiology: tubercle bacillus • Pathogenesis: host hypersensitivity to tubercular protein in pleural tubercles • Delayed hypersensitivity
Clinical Manifestations • Generalized symptoms of toxicity of TB: Fever, high sweat, fatigue and weight loss, etc. • Those of pleural effusion: Pleuritic pain, short breath and dyspnea, etc. • Pleural fluid is exudative and usually reveals lymphocytosis • Rarely pleural fluid is blood stained • The PPD or OT test usually positive
Diagnosis • Based on mentioned findings and some examinations of pleural fluids, and culture of material obtained at biopsy of the pleura and pleural fluids. • except for pleural effusions caused by other causes.
Treatment (1) Standard antituberculous regimens ( usually short course of antituberculous chemotherapy is used ) (2) Administration of corticosteroid during the first several weeks of treatment (3) Thoracentesis
Empyema • Thick purulent fluid with more than 100,000 cells per cubic millimeter or fluid with PH values less than or equal to 7. 20 should be treated as a presumptive empyema • The general objectives of therapy of empyema are the elimination of both the systemic and local infection.
Treatment of acute empyema (1) Control of infection systemic and local (2) Repeated thoracentesis or drainage of the empyema
(3) Chronic empyema is primarily treated operatively (4) Operative therapy is also indicated in the empyema with associated bronchopleural fistula or with the ipsilateral ruined lung.
Treatment of malignant pleural effusion • Use systemic anti-tumor medicines • Local treatments
临床病例 • 病史: • 主诉:发热、乏力、消瘦一月伴咳嗽气急一天 • 现病史:患者于一月前无明显诱因下出现发热,体温高峰38-39℃,以午后始发热为主,同时伴乏力消瘦,一直未予以诊治,于入院前一天出现明显咳嗽和气急,外院胸部X线显示右侧胸部大片密度增高影,纵隔向右侧移位。遂收入院。 • 既往无其他慢性疾病史。
体格检查 • 一般情况:精神差,消瘦, • T:38.3℃, P80次/分,R20次/分,BP90/60mmHg • 胸部体征:望诊:右侧呼吸运动减弱,右侧饱满 触诊:气管向左侧移位,右侧呼吸活动 度减弱,触觉语颤减弱 叩诊:呈实音 听诊:右侧呼吸音消失