Download
1 / 17
180 likes | 429 Views
Choice of chemotherapy in the treatment of metastatic squamous cell carcinoma of the anal canal. Eng C 1 , Rogers J 2 , Chang GJ 3 , You N 3 , Das P 4 , Rodriguez- Bigas M 3 , Ohinata A 1 , Phillips J 1 , Abbruzzese JL 1 , Wolff RA 1

E N D
Choice of chemotherapy in the treatment of metastatic squamous cell carcinoma of the anal canal. Eng C1, Rogers J2, Chang GJ3, You N3, Das P4, Rodriguez-Bigas M3, Ohinata A1, Phillips J1, Abbruzzese JL1, Wolff RA1 The Departments of Gastrointestinal Medical Oncology1, Clinical Pharmacy2, Surgical Oncology3, and Radiation Oncology4, The University of Texas M. D. Anderson Cancer Center, Houston, Texas.
Acknowledgements • Support for this study was provided by an anonymous philanthropic donor, the Farrah Fawcett Foundation, and the E.B. Anal Cancer Foundation.
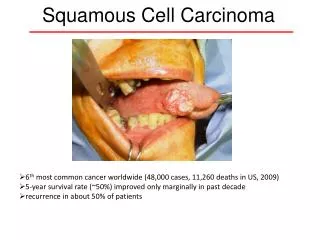
Background • Carcinoma of the anal canal is a rare gastrointestinal malignancy that will affect approximately 6,230 individuals in the United States in 2012, resulting in 780 annual deaths1. • The annual incidence continues to rise, highlighting the need for scientific inquiry into optimal treatment for this disease. • Squamous cell carcinoma (SCCA) represents approximately 85% of all anal cancers2.
Risk factors for anal carcinoma may include a history of HPV infection and chronic immunosuppressed states, i.e., organ transplantation or a history of HIV+. • Notably, in the HIV+ patient population, the use of anti-retroviral therapy has not reduced the incidence of anal carcinoma3. • While greater than 80% of patients typically present with early stage disease,15-20% of patients will develop distant disease4. • Currently, there is a lack of published data regarding optimal management of this malignancy in the metastatic setting, and as such there is currently no standard of care for patients with distant metastasis. • While there is no standard of care, the mainstay of treatment is chemotherapy. Common regimens utilized are those from other more common squamous cell cancers (cervical, head/neck, and lung).
Aim • To evaluate progression-free survival (PFS), overall survival (OS) and response rate (RR) following first-line systemic chemotherapy regimen in patients with metastatic squamous cell carcinoma of the anal canal.
Methods • Study Design and Population (Tables 1 & 2) • Retrospective cohort study of treatment-naive metastatic SCCA patients of the anal canal registered at our institution from 1/1/2000-5/1/2012. • Patients were required to have radiographic imaging at our institution but chemotherapy was allowed to be administered at an outside institution. • Electronic medical records were reviewed for patient demographics, tumor characteristics, and clinical outcomes including: PFS, OS, RR, prior history of STD or immunosuppressed state, prior definitive chemoradiation, histology, systemic regimen, sub-sequent lines of therapy, and treatment intervention for curative intent. • This study was approved by the MDACC IRB. • Statistical Analysis • OS and PFS were determined using the Kaplan-Meier method. The log-rank test was used for statistical comparisons.
Results • 77 treatment naïve patients were evaluable for PFS, OS, and RR. • Median time to development of metastatic disease was 13 months. • After a median follow-up of 42 months: • The median PFS was 7 months for all patients. • The median PFS was greater for PF vs. CP: 8 months (95% CI: 4.5 – 11.5) vs. 4 months (95% CI: 1.7 – 6.3), respectively. • A greater percentage of patients with poorly differentiated histology received CP (67% vs. 45%, p = 0.2). • Median number of chemotherapy cycles received was 4.
The median OS for all patients was 22 months. • Median subsequent lines of therapy was 1. • Patients that received PF were twice as likely to discontinue treatment due to toxicity rather than progression vs. CP (17% vs. 8%). • Treatment with curative intent (N=33) • Type of treatment provided: • Metastasectomy/RFA (48%) • Chemoradiation (43%) • Both modalities (9%) • Median PFS was 16 months (95% CI: 9.2 -22.8) and the median OS was 53 months (95% CI: 28.3 – 77.6).
Conclusions • In the treatment of metastatic SCCA of the anal canal, our analysis suggests that 5-FU/cisplatin may result in improved PFS vs. carboplatin/paclitaxel, but was insufficiently powered to determine superiority, warranting further study. • Selection bias for the chemotherapy regimen may have affected our PFS analysis. Generally, the 5-FU/cisplatin regimen was often provided to patients for whom curative resection might be an option. Whereas, carboplatin/paclitaxel was often chosen for palliation in unresectable patients given the likely toxicities associated with prolonged cisplatin-based therapy.
Notably, our data indicate that whenever feasible, curative intervention can result in worthwhile survival outcomes for metastatic patients. • The short median PFS with front-line therapy, combined with the relatively longer OS reflects the challenges in treating this patient population and the importance of early multidisciplinary management in select cases for curative intent. • We acknowledge the limitations of a retrospective analysis. We nevertheless consider the results worthy of discussion and support consideration for further analysis considering the rarity of this patient population.
References • Siegel et al: Cancer Statistics, 2012. CA Cancer J Clin. 2012 Jan-Feb;62(1):10-29. • Johnson et al: Cancer. 2004 Jul 15;101(2):281-8. • Silverberg et al: CurrOpin HIV AIDS. 2009 Jan;4(1):42-51. • Eng et al: Treatment options in metastatic squamous cell carcinoma of the anal canal. Curr Treat Options Oncol. 2008 Dec;9(4-6):400-7.