Download
1 / 1
10 likes | 304 Views
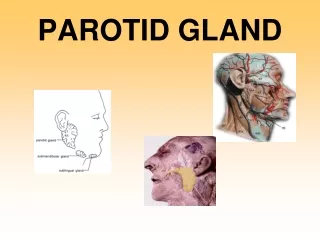
Case Report 54 year old Caucasian female presented with a right asymptomatic parotid mass of 2 month’s duration with no other neck masses nor lymhadenopathy. Fine needle aspirate suggested an epithelial neoplasm.

E N D
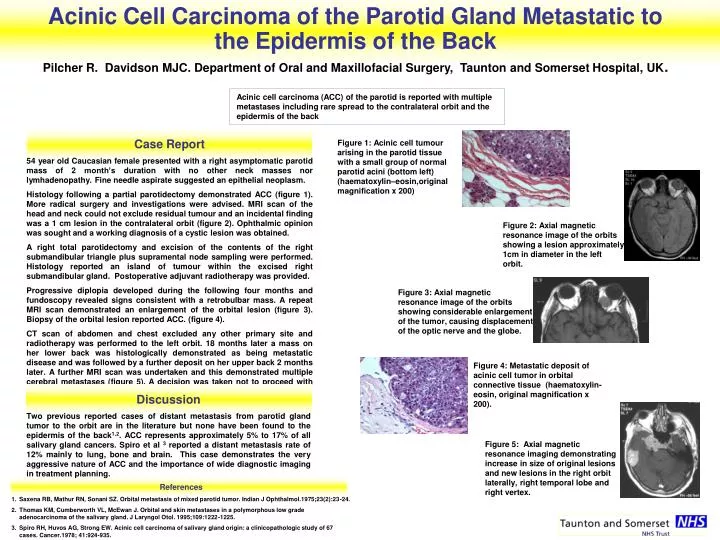
Case Report 54 year old Caucasian female presented with a right asymptomatic parotid mass of 2 month’s duration with no other neck masses nor lymhadenopathy. Fine needle aspirate suggested an epithelial neoplasm. Histology following a partial parotidectomy demonstrated ACC (figure 1). More radical surgery and investigations were advised. MRI scan of the head and neck could not exclude residual tumour and an incidental finding was a 1 cm lesion in the contralateral orbit (figure 2). Ophthalmic opinion was sought and a working diagnosis of a cystic lesion was obtained. A right total parotidectomy and excision of the contents of the right submandibular triangle plus supramental node sampling were performed. Histology reported an island of tumour within the excised right submandibular gland. Postoperative adjuvant radiotherapy was provided. Progressive diplopia developed during the following four months and fundoscopy revealed signs consistent with a retrobulbar mass. A repeat MRI scan demonstrated an enlargement of the orbital lesion (figure 3). Biopsy of the orbital lesion reported ACC. (figure 4). CT scan of abdomen and chest excluded any other primary site and radiotherapy was performed to the left orbit. 18 months later a mass on her lower back was histologically demonstrated as being metastatic disease and was followed by a further deposit on her upper back 2 months later. A further MRI scan was undertaken and this demonstrated multiple cerebral metastases (figure 5). A decision was taken not to proceed with further radiotherapy or to provide chemotherapy. Figure 2: Axial magnetic resonance image of the orbits showing a lesion approximately 1cm in diameter in the left orbit. Figure 1: Acinic cell tumour arising in the parotid tissue with a small group of normal parotid acini (bottom left) (haematoxylin–eosin,original magnification x 200) Figure 3: Axial magnetic resonance image of the orbits showing considerable enlargement of the tumor, causing displacement of the optic nerve and the globe. Figure 4: Metastatic deposit of acinic cell tumor in orbital connective tissue (haematoxylin-eosin, original magnification x 200). Discussion Two previous reported cases of distant metastasis from parotid gland tumor to the orbit are in the literature but none have been found to the epidermis of the back1,2. ACC represents approximately 5% to 17% of all salivary gland cancers. Spiro et al 3 reported a distant metastasis rate of 12% mainly to lung, bone and brain. This case demonstrates the very aggressive nature of ACC and the importance of wide diagnostic imaging in treatment planning. Figure 5: Axial magnetic resonance imaging demonstrating increase in size of original lesions and new lesions in the right orbit laterally, right temporal lobe and right vertex. References 1. Saxena RB, Mathur RN, Sonani SZ. Orbital metastasis of mixed parotid tumor. Indian J Ophthalmol.1975;23(2):23-24. 2. Thomas KM, Cumberworth VL, McEwan J. Orbital and skin metastases in a polymorphous low grade adenocarcinoma of the salivary gland. J Laryngol Otol. 1995;109:1222-1225. 3.Spiro RH, Huvos AG, Strong EW. Acinic cell carcinoma of salivary gland origin: a clinicopathologic study of 67 cases. Cancer.1978; 41:924-935. Acinic Cell Carcinoma of the Parotid Gland Metastatic to the Epidermis of the Back Pilcher R. Davidson MJC. Department of Oral and Maxillofacial Surgery, Taunton and Somerset Hospital, UK. Acinic cell carcinoma (ACC) of the parotid is reported with multiple metastases including rare spread to the contralateral orbit and the epidermis of the back