Download
1 / 15
150 likes | 287 Views
Measuring Health Workforce Distribution Inequalities in Uganda. Anna Awor, Elaine Byrne and Ruairi Brugha. The Challenge. Many challenges: Staff shortages uneven distribution gaps in skills and competencies low retention & poor motivation limited funding for recruitment

E N D
Measuring Health Workforce Distribution Inequalities in Uganda Anna Awor, Elaine Byrne and RuairiBrugha
The Challenge Many challenges: • Staff shortages • uneven distribution • gaps in skills and competencies • low retention & poor motivation • limited funding for recruitment • constricted career structure • Lack of champions for health • lack of recognition & shortage of role models, • ineffective training materials and methods: Without overcoming these challenges, attainment of Millennium Development Goals will not be possible in most developing countries.
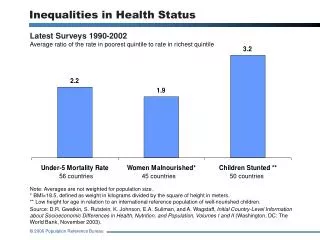
Objective • Assess regional distribution and skill mix of health workers at the Regional Referral Hospitals (RRH) in Uganda, in order to illustrate the imbalances in geographical distribution and skills mix • The analysis was based on the critical HRH levels in the Regional Referral Hospitals
The Ugandan Health System Household/community/village HC II HC III Referral Hospital or HC IV District Health Service Regional Referral Hospital National Referral Hospital MOH Headquarters
Functions of the Regional Referral Hospitals • Preventive, promotive, curative, maternity, in-patient health, and blood transfusion services • Specialist clinical services such as psychiatry, ENT, ophthalmology, higher level surgical and medical, and clinical support • In-service training, consultation and operational research in support of the community-based health care programmes • Teaching and research * each RRH provide services to 2 million people
Methods Using data from the ministry of health HRH audit report 2010, we: • Analysed the distribution of health workers in the 12 regional referral hospitals in Uganda. • Comparedproportions of vacant positions with the set norm for various cadres at the 12 RRH. • Analysed cadre-specific (skill mix) distributions of health workers focusing on the specialised services in the 12 RRH.
Overall Vacancy Rates The health sector strategic plan (HSSP II, 2006-2010) set a staffing level of 65%, of which 4 RRH are lower than this level: • Soroti at 60%, • Fort Portal at 56%, • Kabale at 49%, • Moroto at 31%.
Vacancy Rates for specific cadres • Doctors: vacancy range 0-93% (Jinja, Mbarara: Moroto) • Nurses: -6-60% (Arua, Moroto) • Clinical Officers: -50%-58% (Lira, Hoima) • Anaesthetic Officers: 0-60% (Jinja, Mbarara, Fort Portal : Hoima) • Orthopaedic officers: 17%-92% (Gulu, Moroto)
Discussion • From the rates seen above, it is obvious that medical personnel are carrying out duties for which they are not fully trained, particularly nursing staff and clinical officers. • Equipping these cadre of staff with the relevant skills may be a solution to some of the HR problems faced in the health sector. • BUT they are already overworked ……….
Conclusions • Need innovative solutions. • Task shifting is taking place whether the Ministry of Health wants to acknowledge it or not. • A multi-sectoral approach is required if task shifting is to be effected. It requires: • changes in curriculum • changes in policies • changes in salary scales • The implications of effecting task shifting are not known - need to address this knowledge gap. Otherwise most countries are not eager to tackle the issue.
Ref • Uganda HSSP II, Ministry of health • Human for health audit report 2010; capacity program