Download
1 / 9
90 likes | 254 Views
CASE 1: SYNOVIAL SARCOMA IN CLOSE RELATION WITH RIGHT CERVICO-BRACHIAL PLEXUS 38-year-old female referred to us from our Neurosurgery Service. Previous Clinical history: Hodgkin disease, nodular sclerosis, supradiaphragmatic IIA. Treated with ABVD x 3 and RTP mantle (1997) First symptom/sign:

E N D
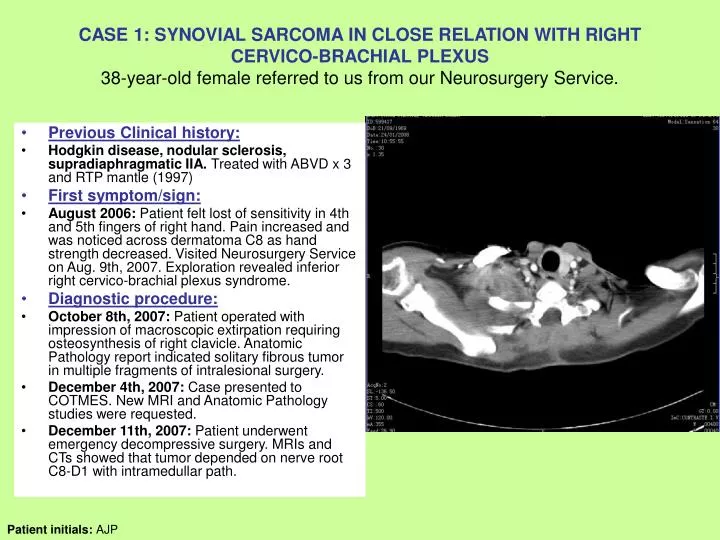
CASE 1: SYNOVIAL SARCOMA IN CLOSE RELATION WITH RIGHT CERVICO-BRACHIAL PLEXUS38-year-old female referred to us from our Neurosurgery Service. • Previous Clinical history: • Hodgkin disease, nodular sclerosis, supradiaphragmatic IIA. Treated with ABVD x 3 and RTP mantle (1997) • First symptom/sign: • August 2006: Patient felt lost of sensitivity in 4th and 5th fingers of right hand. Pain increased and was noticed across dermatoma C8 as hand strength decreased. Visited Neurosurgery Service on Aug. 9th, 2007. Exploration revealed inferior right cervico-brachial plexus syndrome. • Diagnostic procedure: • October 8th, 2007: Patient operated with impression of macroscopic extirpation requiring osteosynthesis of right clavicle. Anatomic Pathology report indicated solitary fibrous tumor in multiple fragments of intralesional surgery. • December 4th, 2007: Case presented to COTMES. New MRI and Anatomic Pathology studies were requested. • December 11th, 2007: Patient underwent emergency decompressive surgery. MRIs and CTs showed that tumor depended on nerve root C8-D1 with intramedullar path. Patient initials: AJP
CASE 1: SYNOVIAL SARCOMA IN CLOSE RELATION WITH RIGHT CERVICO-BRACHIAL PLEXUS38-year-old female referred to us from our Neurosurgery Service. Current situation: The patient has started rehabilitation and the recovery of strength in inferior extremities is MII4+/5 and MID 4-/5. The patient has low cervical pain, possibly related to post-surgery serous and vertiginous sensation in decubitus position. MRI post 2nd operation was requested as well as thoracic-abdominal CT. The case was also reviewed by Pathologists of the CNIO center on December 24th, 2007 in order to confirm or to rule out synovial sarcoma. Thorax and neck CT (January 24th, 2008)
CASE 1: SYNOVIAL SARCOMA IN CLOSE RELATION WITH RIGHT CERVICO-BRACHIAL PLEXUS38-year-old female referred to us from our Neurosurgery Service. CNIO Pathology Report: January 20th, 2007: The cytogenic study through FISH using the probe that detects translocation (X; 18) resulted positive. Morphology and immunohistochemistry study showed very focal positivity for CK. The S-100 expression could also be observed in up to 30% of cases. Diagnosis is monophasic synovial sarcoma. Treatment Plan: Patient started chemotherapy with anthracyclines and ifosfamide on January 28th, 2008. Cervical spine MRI (January 24th, 2008)
Radiology Reports: • Thorax and neck CT (January 24th, 2008): • Endovenous contrast • Tumor with invasion of cervical channel and right brachial plexus • Estimated mass size: 12 x 7 cm • Adjacent supraclavicular adenophaties • 3-mm pulmonar nodule in the inferior left lobule • Cervical spine MRI (January 24th, 2008): • 32 x 30 x 60 mm tumoral mass • Gets into C7-D1intervertebral foramen • Spinal cord compression to left side • Marrow shows edema
CASE 1: SYNOVIAL SARCOMA IN CLOSE RELATION WITH RIGHT CERVICO-BRACHIAL PLEXUS38-year-old female referred to us from our Neurosurgery Service. • Questions: • Pathologist: • Would this case fit in MPSNT (without the translocation study)? • 2. In your experience, have you seen similar cases of synovial sarcoma with close relationship with plexus or peripheral nerves? • 3. Could this be considered as sarcoma induced by radiotherapy? • Oncologist: • Regarding synovial sarcomas, we talked about their special chemo-sensitivity to high doses of ifosfamide. In a metastatic synovial sarcoma, such as this case, would you use as 1-st line standard a combination of anthracycline-ifosfamide? • Surgeon: • What is your experience in tumors with close relationship to cervico-brachial plexus?