Download
1 / 23
240 likes | 286 Views
Explore the physiology of the Renin-Angiotensin-Aldosterone System (RAAS) focusing on Angiotensin, ACE Inhibition, and Angiotensin Receptor Blockade. Learn about the impact on Atherosclerosis, Vasodilation, Prostacyclin, Nitric Oxide, and more.

E N D
VBWG Physiology of RAAS:Focus on Angiotensin
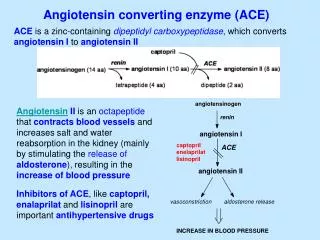
VBWG RAAS: Pathways of ACE inhibition and angiotensin receptor blockade Angiotensin I Chymase,tPA,cathepsin Bradykinin/NO ACE inhibitor Inactivefragments ‘Angiotensin IIescape’ Angiotensin II ARB AT2 receptor AT1 receptor Dzau V. J Hypertens. 2005;23(suppl 1):S9-S17.
VBWG Atherosclerosis-promoting actions of Ang II and protective effects of bradykinin Vasodilation Prostacyclin Nitric oxide tPA Protection against the effects of Ang II Inactive peptides Bradykinin - ACEinhibitor • Vasoconstriction ICAM-1, VCAM-1 • Growth factors • Oxyradical formation • PAI-1 • Smooth muscle cell proliferation • Matrix degradation - • Endothelial dysfunction • Inflammation • Coagulation • Atherogenesis Ang I Ang II Ferrari R. Expert Rev Cardiovasc Ther. 2005;3:15-29.
VBWG Ang II: Influence on structure, function, and atherosclerosis Angiotensin II Growth Thrombosis Smooth musclecell growthand migration Endothelialdysfunction Plateletaggregation Weir MR, Dzau VJ. Am J Hypertens. 1999;12:205S-213S.
ACEI: Proposed continuum of benefits VBWG Immediate onset Blood pressure Bradykinin preservation: NO and vasodilation Intermediate effects Fibrinolysis: PAI-1, tPA Platelet inhibition Long-term effects Cell proliferation and migration Atherosclerotic plaque stabilization Adapted from Bertrand ME. Curr Med Res Opin. 2004;20:1559-69.
Hypercholesterolemia increases angiotensin peptides and atherosclerosis via AT1A receptor VBWG LDL-receptor–deficient mice (LDL receptor–/–) Aortic intimal surface(male) 6 LDL receptor+/+ AT1A receptor+/+ 5 LDL receptor–/– AT1A receptor+/+ 1200 LDL receptor–/– AT1A receptor–/– * 4 1000 Lesionareaofarch (mm2) 800 3 pg/ml * 600 2 ‡ 400 † 1 200 0 0 +/+ –/– Ang II Ang III Ang IV Sum Ang 4–8 Ang 5–8 AT1A receptor genotype Angiotensin peptides *P < 0.001, †P < 0.01 for LDL receptor–/– AT1A receptor+/+ ‡P < 0.001 between genotypes Daugherty A et al. Circulation. 2004;110:3849-57.
Reduction in infarct size with ACE inhibition: Involvement of bradykinin VBWG N = 60 rabbits Normal-fed Cholesterol-fed In this model, AT1 receptor blockade had no effect on infarct size 100 * ‡ ‡ Infarct size (%) † 50 0 Quinapril – – 8 + – 9 + HOE 5 – – 9 + – 8 + HOE 7 + L-NAME 5 n = HOE = bradykinin B2 receptor blockerL-NAME = NO synthase inhibitor *P < 0.05 vs normal-fed †P < 0.05 vs without quinapril ‡P < 0.05 vs without HOE or L-NAME Hoshida S et al. Circulation. 1999;99:434-40. Hoshida S et al. Atherosclerosis. 2000;149:287-94.
ACEI reduces atherosclerosis progression VBWG SECURE 0.025 P= 0.028 0.022 NS 0.020 0.018 Mean maximum IMT slope(mm/y) 37% Reduction 0.015 0.014 0.010 0.005 0 Placebo Ramipril 2.5 mg Ramipril 10 mg Lonn EM et al. Circulation. 2001;103:919-25.
VBWG ACEI may exert anti-ischemic effects in CAD N = 12 ST-segment depression Exercise-induced LV systolic dysfunction 6 P < 0.05 5 –42% P < 0.05 ST-segment changes (mm) 4 2.5 –39% 2 3 LVmotion score 1.5 2 1 1 0.5 0 0 Before 3 months Before 3 months perindopril8 mg perindopril8 mg Morishita T el al. Jpn J Pharmacol. 2002;88:100-7.
VBWG ACEI is associated with less aortic valve calcification 100 P < 0.001 80 75 58 Patientswith AVC scoreprogression (%) 60 42 40 25 No change 20 Progression 0 No ACEIn = 80 ACEI n = 43 O’Brien KD et al. Arch Intern Med. 2005;165:858-62.
VBWG ACEI normalizes structure of resistance arteries in CAD patients Total interstitial collagen Periarteriolar collagen P = 0.04 P = 0.04 800 8 Coronary reserve P = 0.001 600 6 558 ± 270 5.5 ± 3.8 22% µm2 Vv% 4.3 ± 3.2 53% +67% 400 4 Baseline 2.1 260 ± 173 200 2 Perindopril 3.5 0 0 At treatment end (12 mo) Pretreatment (n = 14) Post-treatment* (n = 14) *Perindopril 4–8 mg for 12 months Schwartzkopff B et al. Hypertension. 2000;36:220-5.
VBWG Short term ACEI does not improve transient ischemia in CAD QUinapril Anti-ischemia and Symptoms of Angina Reduction (QUASAR) trial Log rank P = 0.07 Placebo 100 Quinapril 40 mg 80 Level 2 angina(%) 60 40 20 0 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Time (minutes)* N = 336 *Time to induce during exercise treadmill testing after 8-week treatment Pepine CJ et al. J Am Coll Cardiol. 2003;42:2049-59.
VBWG Adipocyte and vasculature interactions Visfatin Adipocyte Angiotensinogen IL-6 TNF- PAI-1 Adiponectin Leptin FFA Insulin sensitivity Insulin resistance Vascular inflammation Endothelial dysfunction Courtesy of W. Hseuh; 2005.
VBWG RAAS blockade increases adiponectin N = 16 with essential hypertension and insulin resistance * • Insulin sensitivity, BMI, and HDL-C independent determinants of adiponectin concentrations • ACEI and ARB increased insulin sensitivity and adiponectin (P < 0.05) • Changes in insulin sensitivity correlated with changes in adiponectin (r = 0.59, P < 0.05) 10 10 * 8 8 6 6 Adiponectin (µg/mL) 4 4 2 2 0 0 Before After Before After Candesartan 8 mg (n = 7) Temocapril 4 mg (n = 9) Furuhashi M et al. Hypertension. 2003;42:76-81. *P < 0.05
ACEI increases tPA release through endogenous bradykinin VBWG Greater effect in women vs men 3 3 *† Net tPArelease(ng/min/100 mL) 2 2 1 1 ‡ 0 0 Vehicle + Enalaprilat HOE 140 + Enalaprilat Baseline Vehicle Baseline HOE 140 Women (n = 7) Men (n = 5) *P < 0.05 vs baseline †P < 0.05 vs vehicle or baseline ‡P < 0.05 vs enalaprilat + vehicle HOE 140 = bradykinin B2 receptor antagonist Pretorius M et al. Circulation. 2003;107:579-85.
Sustained decrease in PAI-1 antigen over time with ACEI vs ARB VBWG 30 20 Week 6 10 PAI-1 antigen (ng/mL) Week 3 Week 1 Week 4 0 –10 –20 AT1 receptor blockade (losartan) ACE inhibition (ramipril) P = 0.043, drug time interaction Brown NJ et al. Hypertension. 2002;40:859-65.
VBWG Greater decrease in PAI-1 over time with ACEI vs ARB 85 Hypertensive diabetic patients treated for 12 weeks P < 0.01 10 5 PAI-1 ng/dL 4 Perindopril 4 mg 0 Losartan 50 mg –5 –10 –10 * Fogari R et al. Am J Hypertens. 2002;15:316-20. *P = 0.028 perindopril vs placebo
VBWG Differing effects of ACEI and ARB on tPA release 25 * 20 * P < 0.05 * * tPA antigen in coronary sinus (ng/mL) 15 * 10 * * 5 0 0 0.2 0.6 2.0 Bradykinin (µg/min) Perindopril 4 mg (n = 16) Losartan 50 mg (n = 15) Control (n = 14) Matsumoto T et al. J Am Coll Cardiol. 2003;41:1373-9. *P < 0.05 vs baseline
VBWG Effects of ACEI on endothelial function: EUROPA substudies • PERTINENT: PERindopril Thrombosis, InflammatioN, Endothelial dysfunction and Neurohormonal activation Trial • Determined the mechanisms by which the ACEI perindopril improved outcomes in patients with stable coronary artery disease • PERFECT: PERindopril-Function of the Endothelium in Coronary artery disease Trial • Evaluated whether long-term administration of perindopril improves endothelial dysfunction Ferrari R. ESC 2004; Munich. Bots ML et al. Cardiovasc Drugs Ther. 2002;16:227-36.
VBWG PERTINENT: Study design EUROPA substudy Objective: Evaluate effects of perindopril on endothelial function and markers of inflammation and thrombosis in EUROPA subgroup of CAD patients Endothelial cell (EC) studies ECs incubated with serum from CAD patients at baseline and at 1 year* Plasma studies Measure substances in plasma that modulate ecNOS and apoptosis Levels measured at baseline vs 1 year Ang II Bradykinin TNF- von Willebrand factor ecNOS EC apoptosis rate *Human umbilical vein ECs ecNOS = EC nitric oxide synthase Ferrari R. ESC 2004; Munich.
ecNOS activity Endothelial cell apoptosis VBWG PERTINENT: Effects of treatment with perindopril for 1 year EUROPA substudy Endothelial cells* Patients’ plasma Ang II Bradykinin TNF- von Willebrand factor • The only significant correlation was between bradykinin and ecNOS • Results suggest perindopril modifies inflammation and thrombosis and endothelial function through bradykinin-dependent mechanisms Ferrari R. ESC 2004; Munich. *Incubated with patients’ serum
VBWG PERFECT: Study design EUROPA substudy Objective: Determine effect of perindopril on brachial artery endothelial function in patients with stable CAD and without clinical HF Design: Double-blind randomized controlled trial Population: N = 333 at 20 centers Treatment:Perindopril 8 mg or placebo Follow-up: 3 years Primary outcome: Change in flow-mediated vasodilation of brachial artery assessed over 36 months Bots ML et al. J Am Coll Cardiol. 2005;45A(suppl):409A. Bots ML et al. Cardiovasc Drugs Ther. 2002;16:227-36.
Mean FMD* increased (baseline vs 36 months) Perindopril 2.7% to 3.3% (+37%) Placebo 2.8% to 3.0% (+7%) Endothelial function (rate of change per 6 months) Perindopril 0.14% (P < 0.05 vs baseline) Placebo 0.02% (P = 0.74 vs baseline) (P = 0.07 for perindopril vs placebo) Conclusion: Part of the beneficial effect of perindopril on CV morbidity and mortality in the EUROPA study may be explained by improvement in endothelial function VBWG PERFECT: ACEI and endothelial function—Preliminary results EUROPA substudy *Brachial artery vasodilation in response to reactive hyperemia Bots ML et al. J Am Coll Cardiol. 2005;45A(suppl A):409A.